











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Foreign accent syndrome (FAS) is a disorder characterized by an affectation in speech automatism. This affectation, since it is expressed with certain motor patterns, is perceived in a biased way by the listeners as a "foreign" accent, although is not associated with previous experience with a second language. 1,2 This interpretation depends on the stereotypes of the listeners regarding particular foreign pronunciations. 3
The syndrome was first described in 1907 by Pierre Marie, who reported the case of a Parisian patient that developed a strong Alsatian accent, along with right hemiplegia. 4,5
The most famous case of FAS is the patient described by Monrad-Krohn in 1947 2,6,7: a 30-year-old woman who developed hemiplegia and global aphasia with agrammatism after suffering from a head trauma with right frontal lesion. During speech therapy, the patient presented an accent that was similar to French, with fluent speech, but without a history of exposure to other languages or learning other languages; her cognitive examination did not reveal any involvement in domains other than language.
Regarding its etiology, the onset of FAS follows cerebrovascular accidents 8 (ischemic or hemorrhagic) or may be a consequence of traumatic brain injuries 9, progressive primary aphasia 10 or multiple sclerosis. 11 In some cases, it begins with total mutism, followed by a limited capacity to moan that leads to articulatory difficulty, described as foreign accent 12, or a clinical profile of prosody alteration, as in cases of cranioencephalic trauma. 9
Despite the heterogeneous presentation of FAS, the cases reported in the literature show some common elements such as distorted prosody, characteristic by which the syndrome receives its name, and awareness of the difficulties experienced, specifically as far as speech production is concerned. 12
Perceived changes in prosody are the result of particular alterations in pitch 6,13, intonation 12,13, duration 14 or other characteristics such as stress 15 and elongation. 16 However, alterations are not limited to prosody; phonetic deviations have been described such as changes in the articulation of consonants or vowels 13,15,17, reduction or simplification of consonant clusters 13,17, and elimination of consonants or vowels. 5,18 Motor aspects of speech are also involved, such as the reduction of production speed. 13,16
The name FAS was coined by Whitaker in 1982. 4 He proposed a set of diagnostic criteria that define neurogenic FAS, where structural injury is the underlying condition. This variation has been especially associated with brain involvement in the dominant hemisphere for language (left hemisphere) 15,19 and subcortical areas 20-22; however, some cases have reported injury in the right hemisphere. 14,23.
Although these criteria shed some light on the diagnosis, they are not always met; consequently, FAS is classified as a neurogenic condition when these criteria are met and as psychogenic 24 or mixed when they are not.
The characteristics of neurogenic FAS are: 1) the patient, their the acquaintances and researchers perceive that the accent has changed, 2) the accent is different from the patient's native dialect before brain involvement, 3) the change in the accent is clearly related to central nervous system damage and, 4) there is no evidence that the patient speaks a foreign language. 4,7,25
Psychogenic, functional or non-organic FAS 13 includes cases in which structural alterations that could explain the symptoms are not observed in the patient. These symptoms occur within the framework of psychiatric disorders such as depression 5, anxiety, conversion disorder 13,26,27, bipolar disorder 28 and schizophrenia. 29,30
Besides these two diagnostic categories, the mixed variant refers organic damage that generates reactive psychological effects such as the emphasis of the new accent. 13
FAS is a complex syndrome that involves multiple levels of speech and that should be approached in a transdisciplinary manner to achieve a better characterization of its presentation and to avoid diagnostic inaccuracies, considering that initial diagnoses such as transient aphasia, larynx disorders or conversion disorder are frequent 1,31 and delay the initiation of interventions.
Speech, language, and neurological and neuropsychological findings of Spanish-speaking patients with this syndrome have not been characterized in detail, unlike the case of English or French-speaking patients. 32,33 Therefore, having such information is essential for clinical and academic purposes.
The following case describes the main neurological, neuropsychological, speech and language findings involved in a Spanish-speaking patient with FAS from a multidisciplinary approach.
CASE PRESENTATION
48-year-old female patient, Colombian, from the urban area of the north of the country, mestizo, from a middle-income household, arts teacher, whose mother tongue and only domain is Spanish. Relevant medical history includes hyperlipidemia and hypertension pharmacologically treated with valsarían, hydrochlorothiazide and amlodipine.
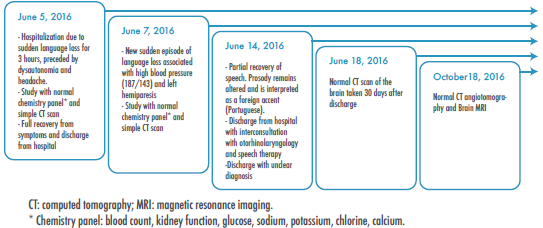
In 2016, the patient presented with a sudden clinical picture of language loss and prosody compromise, with an accent that was recognized as "foreign". The woman was initially treated with speech therapy without having a clear diagnosis. The main symptoms and the clinical evolution are detailed chronologically in Figure 1.
Source: Own elaboration.
Figure 1 Timeline: establishment of the clinical profile and initial approach.
In January 201 7, the patient was referred for assessment by the interdisciplinary neurosciences team of the Universidad Nacional de Colombia (neurology, neuropsychology, phonoaudiology, internal medicine, psychiatry and neuroradiology). The results are detailed in Table 1.
Table 1 Results of clinical assessment carried out by neurology, psychiatry and radiology.
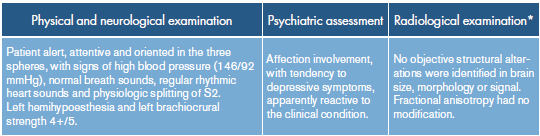
* Multiplanar sequences in 1.5T PHILIPS MULTIVA, TSE T2, SE T1, GRE T1 and T2, including volumetric acquisitions in addition to tractography of 32 directions.
Source: Own elaboration.
The neuropsychological evaluation showed altered performance (22 points) in tasks included in the Moca Test 34, a high subjective memory complaint of the patient and family members 35, and borderline performance 19,5 in the INECO Frontal Screening executive function screening scale. 36 On the other hand, there was evidence of preservation of functionality (score: 14-14), which was measured using the modified Lawton's scale. 37 The evaluation of the cognitive domains attention, memory, language, praxis and executive functions was carried out using the NEURONORMA Colombia battery 38 (Figure 2); language was further evaluated using the guidelines for the assessment of grammatical transformations in Spanish-speaking patients (spontaneous language, evaluation of grammatical elements, agreement with suggested responses, grammatical transformations, construction of sentences, and handling of passive-active constructions and complex structures), and analysis of tasks with linguistic implication and conversational language to establish the state of the different components of language.
Praxis and attentional skills were preserved, although a decrease in processing speed that interfered with the outcome of tasks assessing attention and inhibitory capacity was observed.
Memory capacity was also compromised, since the retrieval of information, both free form and with key, was found to be lower than expected for her age and educational attainment. In addition, the patient presented semantically-related intrusions (4 intrusions).
Further tests were made regarding the language sphere, this being the domain with the most altered report. Figure 2 details the evaluation tests for this domain. Alterations were found in articulation and prosody at the expressive level; speech was abbreviated in short phrases, but it was informative and not telegraphic. Speech was deautomatized, aspect that persisted for automatisms and did not improve in singing tasks. Phonological verbal fluency was diminished and comprehension was correct, as well as denomination. Regarding repetition, reading and writing presented difficulties similar to those observed in oral expression. In addition, writing showed discreet agrammatism, characterized by inappropriate use of adjectives ("my literature is displaced"), difficulty in identifying the right preposition ("there's only time to turn on the forms today") or to preserve singular and plural concordance ("my word are exsaggerated"), and slight alterations of grammatical transformation tasks such as turning nouns into verbs (Beauty-beautiful).
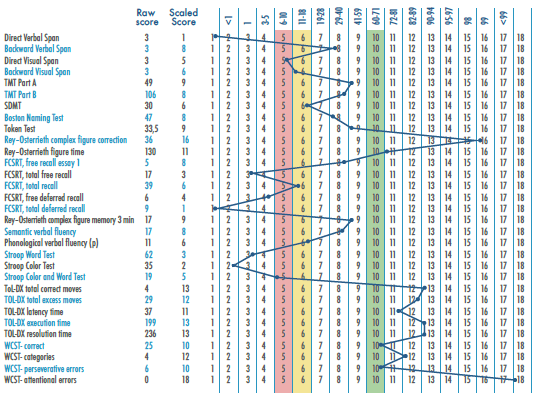
Attention: Direct Verbal Span, Direct Visual Span, Trail Making Test (TMT) Part A and B, Symbol Digit Modalities Test (SDMT), Stroop Color and Word Test, Wisconsin Card Sorting Test (WCST) attentional function. Language: Boston Naming Test, Token Test, Semantic and phonological verbal fluency (p). Memory: Colombian version of the Free and Cued Selective Reminding Test (FCSRT) free recall essay 1, total free recall, total recall, free deferred recall, total deferred recall, Rey-Osterrieth complex figure memory 3 minutes. Building skills: Rey-Osterrieth complex figure correction, Rey-Osterrieth figure time. Executive functions: Backward Verbal Span, Backward Visual Span, TMT B, Phonological Verbal Fluency, (p) Token Test, Stroop Interference Test, Tower of London (ToL-DX) total correct moves, excess moves, latency time, execution and resolution, correct Wisconsin Card Sorting Test (WCST), categories, perseverative errors.
Scores were transformed to scaled measures based on Colombian scales. Decreased performance starting at 1.5 SD (Scaled score 6), indicates alteration if below average. Two or more tests of the same domain below 1.5 SD indicate alteration.
Phonetic analysis
Speech subprocesses were evaluated in detail in the phonetic analysis, finding compromise in different segmental and suprasegmental levels (Table 2).

Diagnostic consensus
From a neurolinguistic and phonoaudiological perspective, and considering that these findings are similar to those reported in the literature 4,15,32,40,41, FAS was diagnosed. MRI and tractography reports helped ruling out structural lesions, neoplasms, ischemic lesions, demyelinating lesions or others brain lesions as a probable etiology of this disorder.
Interventions and recommendations
Controlling comorbidities was the first step in the treatment of the patient. Acetylsalicylic acid was indicated and antihypertensive therapy was adjusted with spironolactone. Rehabilitation included speech therapy for the correction and rehabilitation of movement and coordination of orofacial musculature (tongue, lips, jaw) and diction: point and manner of articulation, allo-phonic substitutions and variations, and systematic vocal articulation exercises. A plan was designed with self-implemented exercises and supervised therapy; it was advised not to resort to group therapy to avoid anxiety.
Cognitive activities were recommended to exercise the involved domains and management with music therapy and permanent intervention by psychiatry and psychotherapy was proposed. In addition, the patient was advised not to abandon her work activities in order to avoid social isolation, although switching to activities that required less oral communication was suggested. Finally, it was proposed to attend control appointments with the treating group.
Follow-up
In the third month of follow-up, speech intelligibility increased by 15% compared to the first measurement, but there was an increase in laryngeal tension and hyperfunctional dysphonia. It was found that the patient maintained the point and manner in the production of occlusive alveolar phonemes, so that instead of /d/ she produced [t], giving silent characteristics to a sonorous phoneme. There was also hypernasalization of the dorsal nasal phoneme (/n/), frontalization of the palatal occlusive phoneme /c/ instead of the alveolar occlusive /t/, omission of the simple vibrant /r/ and centralization of the vowels /dolores/ [doooes].
The maximum phonation time was 4 seconds and expressive language was slightly altered before repetition and denomination. Stereotypes were identified in the production of bilabial occlusive phonemes /b/ and /p/, followed by elongated vowels. A high frequency of phonemic paraphasias /cabeza/ - [aBeta], alterations in melody, segmental pauses (syllabic) and prolongations of vowel sounds with low intensity were observed.
Listening was preserved, although there was evidence of contrasting phonological paraphasias with identified articulatory errors. Mild agrammatism was also evident, but, according to analysis with PRAAT, no variations were identified in the formants F1 and F2.
Alterations persisted between February and April 2017, although there were changes in the accent of the mother tongue with a slight improvement in intelligibility with respect to the initial assessment.
Poor adherence to the intervention recommendations made by the group was documented at 6 and 12 months; this was secondary to the unavailability of specialized management in the patient's place of residence. The assessment made by the treating group did not reveal significant improvement in the clinical condition or in the aspects of speech of the patient during this period.
DISCUSSION
This case reports the neurological and neuro-psychological characteristics of language and speech in a Spanish-speaking patient with FAS. The neurological manifestations that come along with this syndrome in the reported cases are not exclusive to this condition and are mainly associated with brain injury or organic compromise. Motor alterations such as hemiparesis, hemiplegia, facial paralysis 19 and dysarthria 8,42 stand out in this group. However, other alterations such as buccal-facial apraxia 22, gait apraxia 28, ataxia 42, spasticity and lack of coordination 28 have also been described. These signs should be taken into account at the time of conducting a neurological evaluation of a FAS patient.
In the reported case, mild hemiparesis and left hemihypsesia were documented in the absence of structural brain injury in imaging studies; however, it was not possible to rule out functional involvement 28 due to limited access to specialized equipment.
The exploration of speech and language in FAS must be deep and contemplate all the segmental, suprasegmental (speech) and linguistic aspects 32, since all of them may be altered. 41
In this case, there was also evidence of fluctuations in the tone of the voice with occasional tonal breaks and variations in intensity; intrasyllabic duration and frequency of intrasyllabic pauses were increased, similar to what the literature reports. 32,33,43 Articulatory movements were imprecise, slow and with changes in the point and manner of some phonemes and syllables.
In patients with FAS, vocabulary may be restricted, slow production and attenuated prosody may be observed 3, and speech may be similar to mild speech apraxia. 1,16,43 Therefore, in general, verbal expression is characterized by articulatory distortions that affect it 3,32,33, leading to errors that are predominantly phonemic substitutions, laborious articulation, sequential errors and unsuccessful efforts in self-correction. 32,33 These errors are always present and do not depend on the task, so there is no improvement when the patient recites, repeats, reads or exclaims. 13
In this case, the patient showed dissociation between good performance in language tasks that do not directly involve speech and difficulty in tests that evaluate expressive language, compatible with the reported findings 32,33,43 and contrary to what some authors state about the absence of deficits at the level of expressive language, phonetic deformations or lack of fluency, which is usual in motor aphasia. 31
Another sign that may be observed is agrammatism. 3,28,44 Individuals with agrammatism fail to make changes in verb tenses, conjugate verbs, make grammatical transformations and use complex structures. 31 In the study patient, these difficulties were evident mainly at the written level, in addition to disortography and alteration in grammatical compositions such as conjugations, identification of propositions and use of singular and plural.
Regarding the cognitive level, presentation spectrum is variable, while failures may not be observed at all 8 or one or more altered cognitive domains may appear. 19,22,25,28,31,45 The main tasks involved are related to verbal fluency 28,45 and semantics, although failures are reported in tasks such as Stroop (exact but slow performance) 28, backward digit span, problems with tasks that require sustained and alternating attention (TMT A and B) 19,25,45, moderate deficit in reading, slight failures in tests such as Mini-Mental 19 and difficulties in memory tasks. 25,28,46 Specific cognitive tasks such as denomination (Boston test), shortened version of the Token test, repetition of sentences, listening and written comprehension and praxis usually have a normal performance. 12
Cases that show cognitive profiles with failures in tasks that require speed of information processing and working memory have been described 25,28, including those in which FAS develops after cerebrovascular events that present with symptoms that are both dysexecutive and memory-related 28, and whose profile greatly differs from those cases in which FAS is a consequence of injury to the brain stem. 42
Considering FAS as a condition that implies more than an alteration of prosody is fundamental for a proper approach to treatment and rehabilitation. Treatment is specific for each case and should be oriented towards the management of the causes. It is also essential to make a diagnosis of all the cognitive domains involved, without leaving aside the affective and psychosocial sphere of the patients, which should be interpreted according to their context. Considering the absence of structural lesions and the general preservation of cognition, the impact of this condition on quality of life may be deemed as a guide to the objectives that the intervention should address.
In the reported case, an improvement in speech intelligibility was achieved, similar to what is reported in the literature 41; nevertheless, many of the suprasegmental and segmental alterations remained after one year. This could be the result of the lack of adherence to the recommendations due to the difficult access to specialized care in the place where the patient resides, aspects that should also be considered as a factor associated with the prognosis of recovery.
In all cases, a comprehensive management should be ensured from a multidisciplinary and multilevel perspective, in such a way that the personal, family, occupational and social contexts are addressed. 41
CONCLUSIONS
FAS is a complex and rare entity that generates change beyond prosody. Its diagnosis is clinical and based on the manifestations and results of an exhaustive phonetic assessment, but not limited to it.
Other alterations in cognitive functions are present in FAS, especially regarding language, memory and executive functions, and in neurological and affective aspects that should be considered as part of a complete assessment.
Imaging studies and other paraclinicals are not the central axis of the diagnosis and their use is convenient to establish a possible etiology in cases where neurogenic or mixed FAS is suspected.
Clinical characterization is essential for approaching patients with FAS; however, there are psychosocial aspects 47 that should not be neglected, such as the work context or occupation, the place of residence and the support network, as they can become barriers or facilitators to the recovery process.
With respect to this case, it is necessary to highlight the deep linguistic, neuropsychological and clinical exploration carried out in the context of a Spanish-speaking patient. The detailed description of speech elements makes this an interesting case in clinical and academic settings. One of its limitations is the lack of functional studies that could specify the etiology of the condition and guide the classification by type of FAS.
ETHICAL CONSIDERATIONS
The patient accepted the support provided by the research team in order to know the etiology of her clinical condition. She manifested her interest in having her case studied in depth and shared with the scientific community and the general public, as she perceived an inadequate approach to her case as a result of the lack of knowledge of the syndrome by the health personnel during the previous clinical assessments. She is currently undergoing a process of neuropsychological and language rehabilitation aimed at recovering the characteristics of her speech and resuming her work and social dynamics. Additionally, she decided to take courses that allowed her to interact and learn from other activities that promote biopsychosocial well-being.
The patient granted her consent for performing each of the studies, for using the information and publishing the case by signing the informed consent.

