











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
The iliotibial band (ITB) is a flat morphological structure that is made up of connective tissue and is part of the tensor fasciae latae muscle. It extends the fibers of the anterior tensor fasciae latae, and involves the gluteal aponeurosis and the posterior fibers of the gluteus maximus muscle 1 (Figure 1). It originates at the iliac crest, runs parallel to the diaphysis of the femur, inserts at the Gerdy's tubercle -which is located in the anterior and lateral corner of the proximal tibia- and joins the lateral femoral condyle and the tibia. Its functions are to extend, abduct, and laterally rotate the hip, and it is also involved in maintaining posture and lateral knee stabilization.
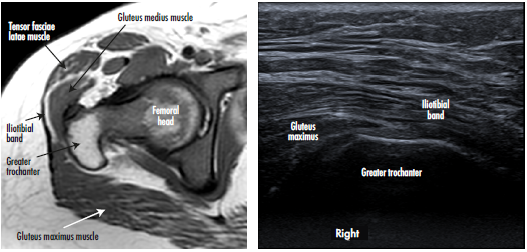
Source: Document obtained during the study.
Figure 1 Magnetic resonance and ultrasound (cross-sectional plane) of the right hip of an asymptomatic patient, where the relationship between the iliotibial band, the tendon of the gluteus maximus and the greater trochanter is evident.
Snapping hip syndrome is a complex condition in which there is an audible noise in the hip when moving (flexion or extension), usually accompanied by pain. 2 This condition was first described by Nunziata & Blumenfeld 3 in 1951; however, in 1995, Allen introduced the term "coxa saltans" to differentiate the causes. 2 At present, three types are described: internal, external (included by some authors in extra-articular) 1,2,4 and intra-articular. The first is caused by the IBT sliding over the femoral head or acetabular ridge, the second by the IBT sliding over the greater trochanter 2, and the third by different causes, mainly degenerative, such as labrum tears, damage to the liagementum teres or loose bodies in the hip. 1,2,4.
The external subtype is the most common type of "coxa saltans" and refers to the snapping sensation caused by a sudden motion of the IBT, whose posterior portion and, to a lesser extent, the distal and anterior portion of the gluteus maximus thicken during hip movements, most frequently during flexion, external rotation and abduction. 1,2,4 During hip extension, the IBT slides over the greater trochanter and returns to the anterior portion during flexion. 2 Pain may or may not be observed during movement, and if it occurs, it coincides with the noise.
External snapping hip syndrome is associated with repetitive physical activities or overuse of anatomical structures related to IBT movements. Some intrinsic risk factors have been identified, such as decreased cervico-diaphyseal angle (coxa vara), the narrowing of the bi-iliac distance, increased distance between major trochanteres, prominence of the major trochanter, and fibrosis of the iliotibial band secondary to multiple intramuscular injections. 5-7
The incidence and prevalence of this syndrome in the general population is not clear 2, although it is usually found in athletes and dancers, with a reported frequency of up to 62% in young women 8, and also in an asymptomatic manner in between 5% to 10% of the population. 9 Affected people visit their doctor because they have difficulty performing common activities such as running, climbing stairs, lifting heavy objects, and even, in some cases, walking. The physical examination is characterized by the reproduction of the noise or palpation of the dislocation during triggering maneuvers: hip flexion and extension.
CASE PRESENTATION
A 29-year-old female patient from Bogotá D.C., with a master's degree in education, white, who works as a psychologist, attended consultation due to symptoms with a year of evolution that began with a sensation of "snap" or prominence in the right greater trochanter, associated with pain, which occurred during walking and when flexing the hip to sit.
Medical history included ligamentous laxity (under study to confirm Ehlers-Danlos syndrome), flexible flatfoot treated with insoles with internal wedge in the hindfoot, length asymmetry in the lower limbs, severe lumbar hyperlordosis, scoliosis from infancy in management with orthosis and Raynaud's phenomenon under study with final diagnosis of vasculitis.
The physical examination showed height of 1.52m, weight of 45k and hypotonic posture caused by lumbar hyperlordosis and thoracic hyperkifosis. The evaluation in standing position revealed tendency to genu valgum with flat foot that compensates with the retraction of the tensor fasciae latae muscle; asymmetry of 4mm in the comparative length of the lower limbs, being greater on the right side; myofascial snapping of the gluteus medius with external extension and flexion hip rotation, without severe hamstring or tensor fasciae latae retraction due to its superimposed hyperlaxity; and significant weakness of the buttocks, predominantly on the right side. Hip impingement and pain were observed when internally rotating the hip bilaterally in a flexed position, especially on the right side, with localized pain in the greater trochanter.
The patient underwent multiple analgesic (until being prescribed with hydrocodone + acetaminophen, which she takes irregularly) and anti-inflammatory treatments, and received multiple physiotherapy sessions without improvement; in fact, her symptoms increased progressively. After assessment by Orthopedics, she was diagnosed with bilateral snapping hip syndrome, with retraction of the tensor fasciae latae. An ultrasound of the hip was performed on both sides, finding thickening of the right tensor fasciae latae (4mm), alteration of the fibrillary pattern and tendon protrusion over the greater trochanter during dynamic assessment, accompanied by an audible and palpable "snap" (Figure 2) (Video 1). Magnetic resonance imaging (MRI) of the hip showed bilateral edema of the ITB and slight thickening of the ITB on the right side (2.3mm) (Figure 3).
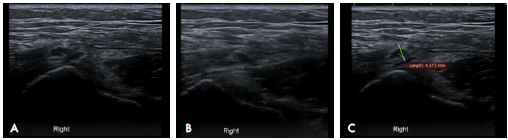
Source: Document obtained during the study.
Figure 2 Dynamic ultrasound of the iliotibial band over the greater trochanter. A) neutral position of the right hip; B) hip internal rotation; C) thickening of the iliotibial band measured in the transverse plane associated with heterogeneous echogenicity of the tendon.
Source: Document obtained during the study. Note: Dear reader in order to watch the video you need to download the PDF file and open it with Acrobat Reader (having previously installed the Adobe Flash Player add-on) and click on the video once. Source: Document obtained during the study.
Video 1 Dynamic ultrasound of the iliotibial band over the greater trochanter before the patient underwent the surgical procedure.
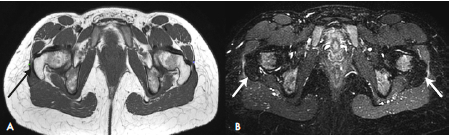
Source: Document obtained during the study.
Figure 3 Magnetic resonance imaging. A) Enhanced axial T1-image showing slight thickening and undulation of the right iliotibial band (black arrow); B) axial plane with Short tau inversion recovery sequences, where an increase in signal intensity of the iliotibial band is identified on both sides (white arrows).
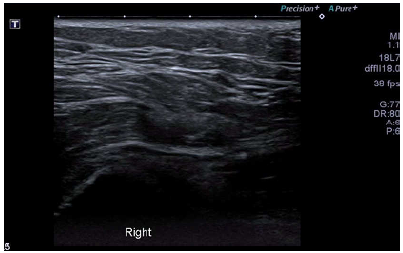
Two years after the onset of the symptoms, the patient required an arthroscopy, so a T-shaped incision of the ITB was made in the right hip using radiofrequency. During a second surgery, an X-shaped incision was made in the fasciae latae muscle on the left side, also by radiofrequency, with subsequent formation of a rhombus and fixation. The patient presented recurrence of predominant symptoms in the right hip. A control ultrasound was performed again, showing greater tendon thickening and peritendinous fluid, probably of post-surgical origin (Figure 4) (Video 2).
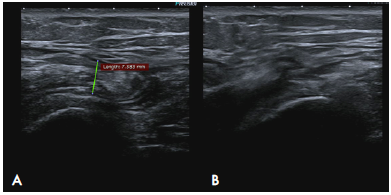
Source: Document obtained during the study.
Figure 4 Ultrasound of the patient taken during post-surgical control 1 month after iliotibial band release. Persistence of symptoms. A) Increase in the thickness of the right iliotibial band (7.5 mm) with respect to the initial ultrasound. B) Dislocation of the iliotibial band during hip external rotation.

Source: Document obtained during the study. Note: Dear reader in order to watch the video you need to download the PDF file and open it with Acrobat Reader (having previously installed the Adobe Flash Player add-on) and click on the video once.
Video 2 Ultrasound of the patient taken during post-surgical control 1 month after iliotibial band release.
One year after the first surgery, the woman underwent a new surgical procedure on the right hip, consisting of ITB opening, partial synovectomy and tenotomy of the hip at two levels, and proximal and distal release. Severe tendon fibrosis secondary to previous surgical procedures was reported as an additional finding. At the time of completion of this case report, the patient had shown partial improvement of the symptoms and had not undergone any new imaging controls.
DISCUSSION
The main structure involved in external snapping hip syndrome is ITB; however, to a lesser extent, there may also be involvement of the tendon of the gluteus maximus. 10 Although the diagnosis is mainly clinical, diagnostic images allow ruling out other causes of hip pain such as bone or soft tissue alterations, bursa, labrum tear, among others. The most widely used and useful modality is dynamic ultrasound. Simple x-rays are usually normal, but allow ruling out intra-articular causes of this syndrome. There is still no consensus to determine diagnostic parameters. 2,11
Dynamic ultrasound shows thickening of the iliotibial band and heterogeneous echogenicity of the fibers, as well as secondary findings such as distension of the greater trochanteric bursa. This dynamic evaluation is useful since it verifies movement of the ITB or the tendon of the gluteus maximus on the greater trochanter, and allows perceiving the dislocation or listening to the "snap", thus leading to the definitive diagnosis of this syndrome. 2,4
The appropriate tool to perform the dynamic ultrasound evaluation is a high frequency linear transducer (12 MHz or higher), with the patient in supine or standing position. Based on the radiologist's preference, the transducer is placed transversely to the greater trochanter, and the exploration is performed with active and passive flexion and external rotation maneuvers of the hip. The abrupt displacement of the ITB or the gluteus maximus muscle is related to the painful "snap" perceived by the patient. 4,7
According to the literature, the MRI findings include thickening of the iliotibial band (>2mm) and of the anterior edge of the tendon of the gluteus maximus (>2mm), with undulation of the contours of both structures 7; the signal is hypointense in T1 and hyperintense in T2. Inflammatory changes of the greater trochanter bursa, visualized as a hyperintense T2 collection, and peritendinous enhancement following administration of intravenous contrast medium can also be seen; however, these findings are nonspecific and should always be analyzed bearing in mind the patient's clinical features. 1 Retrospectively, ipsilateral gluteus maximus atrophy has been identified as an additional finding of this syndrome. It is important to enlarge the field of vision in order to fully visualize the region of interest: this includes the entire pelvis and its soft tissues.
Computerized tomography permit a better evaluation of bone structures, while the multi-planar reconstructions that can be carried out allow better characterizing the findings that predispose to the snapping hip syndrome, and ruling out intra-articular causes. This study should not be the first choice as the resolution of the soft tissues is not good. 8
Taking into account the findings of the present case, a dynamic ultrasound was the diagnostic modality that best allowed evaluating the patient and corroborating what was identified during the physical examination. Besides identifying the key finding, which was the subluxation of the ITB over the greater trochanter accompanied by pain, changes in the soft tissues (in the second ultrasound) were found that could explain the persistence of symptoms.
Treatment in these patients includes rest, physical means (local heat), stretching exercises, release of loads during daily activities, and analgesics and non-steroidal anti-inflammatory drugs. Conducting anesthetic or corticosteroid infiltration of the trochanteric bursa or iliotibial band has been proposed if there is no response. 8
When there is no response to conservative treatment, surgery should be done in order to eliminate tendon protrusion. Possible surgical procedures include resection of the major trochanteric bursa, trochanter osteotomy and, in refractory cases, arthroscopic release of the ITB or lengthening of the ITB by Z-plasty. 1,2
The failure of surgery in the reported case is still cause for study. Specialists believe that the recurrence of symptoms may be associated to a marked fibrotic process following the two surgical procedures; however, that baseline hyperlaxity may be associated with recurrence of symptoms is considered a possibility.
CONCLUSIONS
This case report describes the ultrasound and MRI imaging findings of external snapping hip syndrome, which allow radiologists to recognize and contribute to the management of this pathology in a timely manner.
Dynamic ultrasound is the most useful technique for the diagnosis of snapping hip syndrome, as it allows confirming the main finding, which is the protrusion of the ITB or the tendon of the gluteus maximus over the greater trochanter. Other techniques, such as x-ray and MRI, provide secondary information on possible differential diagnoses of painful hip or help rule out the intra-articular variant of this syndrome.

