











 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Epstein-Barr virus (EBV) was described in 1964 in cell cultures from Burkitt lymphoma samples; however, infectious mononucleosis is the clinical syndrome most frequently associated with this infection. 1,2
EBV, or human herpesvirus type 4, belongs to the Herpesviridae family, Gammaherpesviridae subfamily, and is the prototype for the Lymphocryptovirus genus. It has a double-stranded 172kb DNA encapsulated in a 100nm icosahedral capsid that protects genetic information, and surrounds itself with a complex proteolipid envelope. To date, only 2 types of this virus have been identified: EBV-1 and EBV-2. 1,2
Its role as an infectious agent in eye pathologies is still little known, since 95% of the healthy population has positive antibody titers; it is only observed in immunocompromised patients with rare severe ophthalmological involvement. Occasionally, conjunctivitis or uveitis may occur, although some other herpesviruses, such as herpes simplex and varicella-zoster virus, may cause retinal involvement with necrosis. 3-5
EBV has been ascribed several ophthalmological pathologies, including multifocal choroiditis and, in the presence of systemic infections, all segments of the eye are involved. Ocular manifestations related to EBV infection may range from oculoglandular syndrome to conjunctivitis, dry eye syndrome, keratitis, uveitis, choroiditis, retinitis, ophthalmoplegia, or papillitis; specifically, conjunctivitis, dacryoadenitis, epiescleritis, keratitis, and iritis are observed in the anterior segment. Reported neurological complications include papilledema and optic neuritis. 5,6
Retinal involvement is rare in cases of EBV associated with infectious mononucleosis; however, a variety of presentations, including retinochoroiditis, have been associated with systemic disease. Definitive evidence of EBV with acute retinal necrosis or vasculitis is scarce and has few cases reported in the literature. 3-6 Retinitis is a cause of impaired visual acuity, which should lead to differential diagnosis given its impact on patients with human immunodeficiency virus (HIV) infection. 3-6
Based on the above, the objective of this report is to present a case of retinitis by EBV in an immunocompetent young adult patient, highlighting, on the one hand, that this presentation is rare in this population group and, on the other, the success of treatment with Aciclovir despite the little evidence available in the literature.
CASE PRESENTATION
An 18-year-old male, high school student from Bogotá D.C., Colombia, white, of a middle-income household, was treated at a quaternary care hospital in December 2017 for symptoms characterized by loss of visual acuity and myodesopsia in the right eye, which appeared suddenly three months earlier. Since the onset of symptoms until the time of consultation, the man was empirically managed with Acyclovir at a dose of 400mg every 12 hours with partial improvement of symptoms; the dose was adjusted to 400mg every 4 hours by indication of the Infectious Diseases Service in December 2017.
In the initial ophthalmology evaluation, the external eye examination was normal in both eyes; biomicroscopy showed clear cornea, well-formed anterior chamber, round central pupil and normal iris in both eyes. Ocular pressure was 12 in both eyes, and the lens was transparent in both eyes. Retina and vitreous body examination showed retinal detachment with abundant subretinal hemorrhage in the lower region and mild vitreous hemorrhage with macular involvement in the right eye. The initial visual acuity of the right eye was 20/400, and 20/20 in the left.
One month after the onset of symptoms, during the second ophthalmology evaluation, the visual acuity of the right eye was 20/200 and of the left eye, 20/30, with biomicroscopy of the right eye that showed grade 2 vitreous hemorrhages and subhyaloid hemorrhage with temporary exsanguinated vessels in the inferior nasal quadrant in the periphery, pale colored macula with exsanguinated vessel in the inferior temporal arch, and difficult detail of the papilla. The subhyaloid hemorrhage also presented with temporary intraretinal hemorrhages, so a possible infectious etiology was considered; management was initiated with Aciclovir at the doses described above.
In October 2017, an ocular ultrasound showed severe low and medium reflectivity vitreous opacities with denser membrane formation in the lower quadrants, posterior vitreous detachment with inferior traction and severe subhyaloid opacities; the head of the optic nerve had normal appearance, so a picture compatible with severe vitritis, mixed opacities suggestive of bleeding areas, and inferior traction of the retina was considered.
Because of the reported changes, the patient was taken to subsequent vitrectomy with endolaser plus air for diagnostic purposes in order to take samples for PCR (polymerase chain reaction), cytomegalovirus (CMV), herpesvirus and EBV processing, by means of the LightMix technique using primers for EBV and specific probes. 10 copies of the amplified gene were obtained, being positive from cycle 31.4, which led to consider the sample as positive for EBV. No intravitreal treatment was provided. The remaining results are shown in Table 1.
Table 1 Vitreous humor tests using the PCR technique.
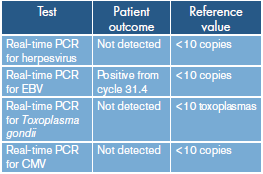
PCR: polymerase chain reaction; EBV: Epstein-Barr virus; CMV: cytomegalovirus.
Source: Own elaboration.
In November 2017, different tests were carried out to rule out immunodeficiency disorders or other concomitant conditions that explained the symptomatology, but they were negative (Table 2).
Table 2 Blood tests.
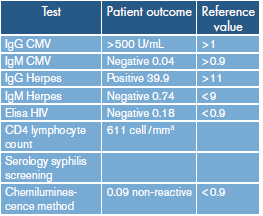
CMV: cytomegalovirus; HIV: human immunodeficiency virus.
Source: Own elaboration.
Also in November 2017, fluorescein angiography of both eyes was performed (Figure 1), which showed mild media opacity in the right eye, poorly defined optic disc, fibrovascular proliferation in the optic disc area and the lower area, adequate filling and transit of the dye through retinal vessels since the beginning, with hyperfluorescence observed in the optic disc that increased as the angiographic transit progressed. Given the findings, a treated viral vasculitis was considered with secondary viral neovascularization and persistence of proliferative activity with suspicion of diffuse macular edema, the latter according to the reading of the retina specialist.
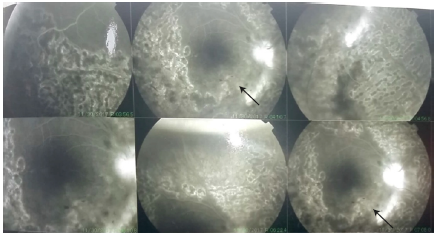
Source: Document obtained during the study.
Figure 1 Findings of fluorescein angiography in the right eye. → Fibrovascular proliferation in the area of the optical disc and in the lower area.
Finally, the patient was followed by the Infectious Diseases Service on a monthly basis from December 2017 to February 2018. The evolution was satisfactory, so management with Aciclovir was suspended after almost 6 months of treatment. The young man presented complete resolution of right eye symptoms with evolution of visual acuity to 20/40 with respect to initial values of 20/400. This case was considered as retinal vasculitis by EBV with adequate therapeutic response to Acyclovir despite having few literature data on doses and duration of management. This could be the first case reported in Colombia so far.
DISCUSSION
This paper reports a case of unilateral retinal vasculitis due to EBV in an immunocompetent young adult, who was successfully treated with Acyclovir for 6 months with complete resolution of symptoms and almost complete improvement of visual acuity. In spite of having insufficient initial doses of the drug, almost complete resolution of the symptoms was achieved after the adjustment.
The cases previously described in the literature on EBV retinitis only describe inflammation of the posterior pole, which contrasts with the reported case of generalized vasculitis of the eye with retinal detachment. This symptomatology is not an ocular manifestation of this virus as frequent as the involvement of the anterior chamber. 5-8 It is important to point out that this is a young patient without HIV infection, condition that is closely related to severe ocular involvement.
The pathogenic capacity of EBV is well known, and it can also cause intraocular inflammation and acute retinal necrosis 9; however, given its ubiquity, it has also been associated with multiple ocular pathologies ranging from mild conditions to severe impairment of visual acuity with retinal detachment, as in the case presented here. All this has been described in both immunocompetent and immunocompromised patients, especially HIV-infected patients where EBV and CMV are responsible for severe necrotizing retinitis. 10,11
The diagnosis of intraocular infection by EBV and other herpesviruses is based on molecular tests that, in this case, were performed in vitreous humor with real-time polymerase chain reaction (RT-PCR). Although genotype detection is not available, this was the only positive test and was, therefore, considered a confirmed case of EBV retinal vasculitis. 3,12
Appropriate management of an unknown condition, as is the case of eye involvement by EBV, is unclear because there are no clinical trials of this type of case. Virus identification leads to the use of antivirals, especially in patients with high viral load, study that was not performed in the reported patient. 13
Andersson et al.14 found a significant decrease in the spontaneous growth of EBV-infected B lymphocytes in vivo after Acyclovir therapy, but given the poor number of cases analyzed, the use of this medication is considered debatable. The review by Rafailidis et al.13 suggests that antiviral agents could be considered for severe manifestations of EBV infections, including meningitis, meningoencephalitis, cerebritis, peripheral nerve palsy, myocarditis, hepatitis, and hematopoietic or kidney disease in immunocompetent patients, as well as an adjunct to steroid treatment. Nevertheless, there is no description of management with antivirals for eye involvement, only one case described by Keorochana 12 in which the use of antivirals showed a similar result to that obtained in the present case. It remains to be established whether joint use with steroids decreases the progression of the pathology and whether it is determinant in visual loss in these cases.
It is not possible to define if management with oral Acyclovir is the best therapeutic option, given that this is a single case and there is no extensive documentation of case series or clinical trials with other antivirals or intravitreal medication, which was not done in this case and leaves open the possibility of using such a strategy in the management of this pathology.
Eye involvement by EBV may include all segments of the eyeball. Cases reported so far include conjunctivitis, dacryoadenitis, episcleritis, keratitis, iritis, and optic nerve neuritis. In addition, Keorochana 12 reported their most recent case of involvement by retinal vasculitis, suggesting eye involvement with decreased visual acuity.
EBV should be considered within differential diagnoses, even in immunocompetent patients, leading to the implementation of vitreous humor sampling since, as in this case, as this was the only way to obtain the diagnosis.
CONCLUSIONS
PCR allowed the diagnostic confirmation of retinal vasculitis by EBV, which demonstrates the importance of vitrectomy, even with therapeutic intent. The patient had an adequate response to Acyclovir despite the disagreements regarding its use and the different doses received. This is the first case of this type reported in Colombia so far.
In spite of the fact that this is a single case, there were limitations such as access to the clinical history of the patient and vitrectomy - which was performed for taking samples only-, and the fact that treatment with Acyclovir was sometimes empirical. The present report shows the importance of reporting similar cases in order to determine specific treatments and procedures to be carried out when eye involvement with a suspicion of infectious origin is found.

