











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Adult Onset Still's disease (AOSD) is a rare inflammatory disease of unclear origin. Its incidence and prevalence vary according to the geographical area: 0.16 to 0.4 cases per 100 000 population and 1 to 34 cases per 1 000 000 population, respectively. 1 This is a disorder that affects men and women alike. 2,3
Although the pathogenesis of AOSD is not entirely clear, it has been suggested that it is an uncontrolled inflammatory response in the form of a "cytokine storm" that occurs when individuals with non-inherited genetic susceptibility associated with different genes of human leukocyte antigen and polymorphisms in genes coding for interleukin 18 (IL-18) and macrophage migration inducer are subjected to a trigger or "second hit" such as viruses, bacteria, and hematological, or solid tumors. Such a response would cause the multi-systemic symptoms associated with the disease. It should be noted that, even though this is one of the most widely disseminated hypotheses, it is still debated. 4,5
AOSD is a little known disease that is not included in the initial differential diagnosis of the febrile illness, leading to a delay in the diagnosis, the initiation of unnecessary pharmacological treatments that may cause adverse effects, and costly complementary studies that are not useful or comfortable for the patient.
This disease is characterized by a triad of fever, evanescent maculopapular exanthema and arthralgia:
Fever is generally high (>39°C), with a double quotidian pattern, and usually increases in the evening and at night. This clinical sign tends to resolve on its own or rapidly with antipyretics and precedes the onset or exacerbation of other systemic symptoms. 6,7
The exanthema typically described in the literature is an evanescent salmon-pink maculopapular rash, occasionally pruritic, predominantly on the trunk and proximal parts of the limbs. Atypical presentations with urticarial exanthema or with persistent erythematous plaques and papules have also been described. 8
Multiple joints may be initially involved, predominantly the knees, ankles, and wrists, with subsequent progression to small joints.
Other manifestations of AOSD include odynophagia, splenomegaly, lymphadenopathy, and hepatomegaly. 7,9
Macrophage activation syndrome is the complication most associated with AOSD, followed by disseminated intravascular coagulation, thrombotic thrombocytopenic purpura, and diffuse alveolar hemorrhage. Other less known complications with isolated case reports are serositis, pericardial effusion, pleural effusion, abdominal pain, pulmonary involvement, myocarditis, 10 and neurological and kidney complications.
Multiple criteria lead to the diagnosis of this disease; however, the Yamaguchi criteria are the most sensitive. To diagnose AOSD, five or more criteria must be met, and two of them must be major. The greatest limitation to the application of the Yamaguchi criteria is the need to rule out infectious processes, neoplasms and systemic rheumatological or inflammatory pathologies that produce the same symptoms. Other criteria for the diagnosis of AOSD are the Fautrel and Cush criteria, which are less known and barely used (Table 1). Currently, the course and treatment of the disease are determined based on whether the patient has a predominant systemic pattern or a joint pattern. 11
Table 1 Classification criteria for Adult Onset Still's Disease.
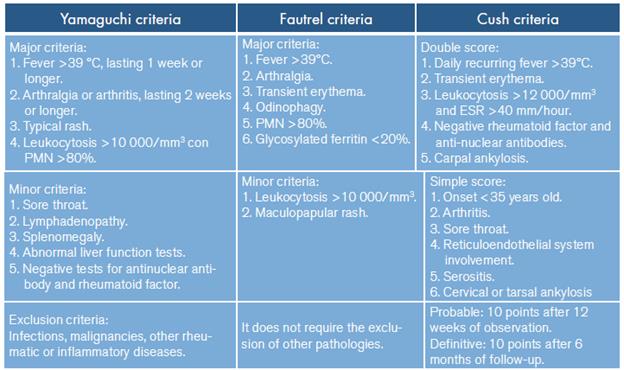
PMN: polymorphonuclear cells; ESR: erythrocyte sedimentation rate.
Source: Elaboration based on Giacomelli et al.1 y Li et al.2
The first-line treatment for AOSD involves anti-inflammatory drugs and steroids. In 60% of the cases, the disease is controlled with glucocorticoids, and patients who do not respond to this therapy may be treated with disease modifying drugs, including methotrexate, which is the one with more evidence. 1 Biologic response modifiers are recommended in cases where the first or second line of treatment does not work, or in patients with contraindications to the use of these drugs. When the pattern is systemic, medications are initiated to control IL-1 B (anakinra, canakinumab, or rilonacept) and IL-18 (tadekinig); if the condition has a predominantly joint pattern, anti-IL-6 (tocilizumab) and anti-TNF (etanercept) therapy should be initiated.
CASE PRESENTATION
This is the case of a 32 year-old female patient with no relevant medical history, mestizo, single, with complete high school education, head of household, mother to two adolescents, worker in a flower farm, from a rural area of a municipality of Cundinamarca (Colombia) located at 2 580 m.a.s.l. The patient was admitted to the hospital after being referred from a primary care center because of a 15-day history of prolonged febrile illness without a clear description of the pattern. She presented migratory polyarthralgias, predominantly in wrists and ankles, and intermittent pruritic salmon-pink macular exanthema mainly in the trunk, upper limbs and proximal part of lower limbs; according to the patient, the exanthema appeared after experiencing febrile peaks, myalgias and intense odynophagia.
The patient had been previously treated with a single dose of intramuscular benzathine penicillin for suspected tonsillopharyngitis caused by Streptococcus pyogenes. Moreover, five days before being admitted, she was hospitalized and treated with antibacterial spectrum of ampicillin/sulbactam for suspected urinary tract infection; since she did not respond to the treatment and the fever peaks and leukocytosis persisted, she was transferred to be assessed by the internal medicine service.
No fever or changes in vital signs were reported in the initial physical examination. There were no signs of an inflammatory process in the tonsils, but painless and mobile posterior cervical lymphadenopathies were palpated, and pink exanthemas that disappeared under pressure were observed on thighs and forearms. Upon admission, studies were initiated for fever of unknown origin (FUO), antimicrobial and antipyretic management was suspended, and analysis was oriented towards neoplastic, inflammatory, rheumatological and infectious causes that could explain the symptoms referred by the patient.
Initial laboratory tests showed a hemogram with a marked increase in the leukocyte count (25 750 leukocytes/mm3) and predominance of polymorphonuclear cells (93.5%). Moreover, the levels of C-reactive protein, aspartate aminotransferase and alanine aminotransferase were 25.4 mg/dl, 70.5 U/L and 228 U/L, respectively. A chest X-ray was taken, revealing an unclear image of retrocardiac alveolar infiltrate (Figure 1). Based on this initial profile, and since the patient completely denied any respiratory or urinary symptoms, additional blood chemistry tests and a thoracoabdominal CT scan were ordered to rule out solid tumors and lymph node involvement.
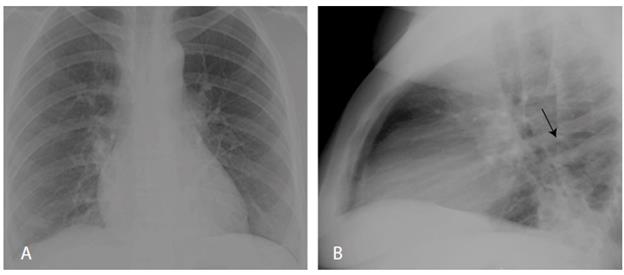
Source: Document obtained during the study.
Figure 1 Chest X-ray on patient's admission. A) anteroposterior plane without evidence of relevant alterations; B) lateral plane with segmental atelectasis.
During hospitalization, the patient presented with feverish peaks >39°C at around dusk and at night, which made the limb exanthema more noticeable and responded quickly to management with non-steroidal anti-inflammatory drugs. Additional tests ruled out infections by human immunodeficiency virus, syphilis, hepatitis B and hepatitis C; the thick blood smear was negative for hemoparasites, the globular sedimentation rate was established at 48 mm/hour, lactate dehydrogenase was 431.7 U/L, and the peripheral blood smear did not report alterations in red cells or platelets, but indicated elevated white blood cell count with neutrophilic predominance.
Based on the reported management that the patient received prior to her arrival at the hospital, diagnostic suspicion began to shift towards AOSD or, less likely, acute rheumatic fever. Tests for antinuclear antibodies, rheumatoid factor, and antistreptolysin were negative, as were blood cultures for aerobic or anaerobic bacterial growth. An echocardiogram was performed, ruling out subclinical carditis, which was described in the 2015 revision of the Jones criteria for rheumatic fever. 12,13 Given the persistence of the febrile peaks and considering the CT scan results, antimicrobial treatment was restarted using antipseudomonal penicillins; however, the patient continued experiencing febrile peaks and elevated leukocyte count in control hemograms. Days later, the official report of the chest tomography ruled out infectious processes but described bilateral pleural effusions with underlying passive segmental atelectasis (Figure 2A). The abdominal CT scan report documented mild nonspecific edema of the gallbladder walls and a small amount of free fluid in the posterior pouch and iliac fossae (Figure 2B); the official report ruled out infectious and neoplastic processes at the thoraco-abdominal level, so antibiotic therapy was suspended.
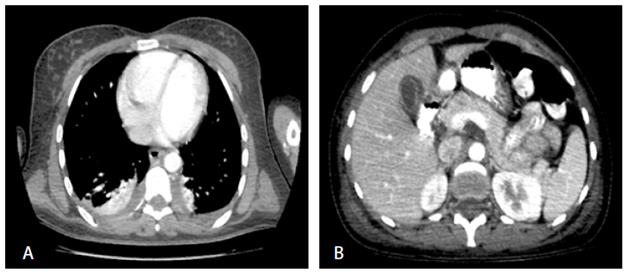
Source: Document obtained during the study.
Figure 2 CT scans. A) Axial plane of the lungs showing pleural effusion associated with atelectasis; B) Axial plane of the abdomen with evidence of an inflammatory process in the gallbladder that is not associated with calculi.
Finally, based on the elevated serum ferritin values (1650 ng/mL) and following the Yamaguchi criteria, AOSD was diagnosed and first-line management with oral prednisolone at a dose of 0.8 mg/kg/day was initiated. After 72 hours, the patient's condition improved, no new febrile peaks were observed, and her arthralgias were controlled. She was subsequently discharged with steroid treatment, calcium supplementation due to the known effect of corticosteroids on ion metabolism, and orders for outpatient follow-up by the internal medicine service.
At the time of preparation of this case report, telephone, and she reported no worsening of the patient's progress had been monitored by symptoms or adverse reactions.
DISCUSSION
AOSD is a rare inflammatory disorder whose incidence and prevalence have not been reported in Colombia. This is an understudied disease that is generally not considered in the initial differential approach to patients with prolonged febrile syndrome given the limited knowledge of its clinical manifestations and treatment, even though it is a common documented cause of FUO.
The case presented here illustrates, precisely, the typical diagnostic triad of the disease: febrile peaks, posterior exacerbated exanthema, and joint involvement in the appendicular skeleton, in addition to the characteristic serological bio-markers. Furthermore, as a novelty, the patient presented with an inflammatory process in the gallbladder, which was not associated with calculi and had not been previously reported; this is an incidental finding that serves as a precedent for follow-up in future cases related to this pathology. This case is an example of the procedure and diagnostic method used for this disease, which is within the group of pathologies to be ruled out in the diagnosis of FUO according to the definition originally proposed by Petersdorf and Beeson, cited by Cunha et al.14
Regarding the available literature on AOSD, there are multiple articles worldwide on new findings concerning its pathogenesis, course, clinical markers, and treatment. 15,16 In Latin America, mainly in Brazil, Argentina, Chile, and Peru, there are a large number of case reports about its typical and atypical characteristics, and its more common complications. 17-20 Specifically in Colombia, updated literature is scarce, and there are only two retrospective studies on case series that analyze the response to monotherapy and combined treatment, 21,22 namely, a review article on its history and pathophysiology 23 and a case report that briefly describes the diagnostic process. 24 It should be noted that there is an additional report of a Colombian case published abroad. 18
This case report attempts to provide more detailed and meticulous information about the diagnosis of AOSD by exposing the complexity of this process and highlighting common errors in the interventions performed on patients. Similarly, it stresses the importance of considering this pathology as a possible cause of the febrile syndrome and the fact that it is not necessary to carry out specialized laboratory tests to make the initial approach to the patient; in fact, a good anamnesis could lead to the suspicion of this disease and prevent the indiscriminate use of antibiotics or other types of interventions.
The authors consider that the publication of this typical case of AOSD contributes to the description of the classic characteristics that guide the diagnosis of the disease and to enrich the Colombian and world literature on the subject, since there are still large gaps in terms of diagnostic tools for this disease in which further research is needed.
CONCLUSION
Although a wide variety of laboratory tests and advanced imaging are available today, the patient's medical history and a detailed physical examination remain the cornerstone of AOSD diagnosis, making it a challenge to physicians. In this sense, the case presented here demonstrates the difficulty of its diagnosis and the importance of its early recognition to avoid complications and improve the prognosis of patients.
PATIENT'S PERSPECTIVE
The patient had trouble during her hospital stay due to the length of her stay and uncertainty about her diagnosis. In addition, the woman had concerns about her financial responsibilities as a stay-at-home mother and anxiety about being away from her children, so she required support from the psychology service in order to cope with her condition and the hospital management.

