











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Pentalogy of Cantrell was first described in 1958 when Cantrell et al.1 published a series of five cases about this abnormality. It was defined as a collection of four midline body defects (specifically in the abdominal wall, sternum, diaphragm, pericardium and heart) accompanied by some intracardiac defect 2. Regarding intracardiac abnormalities, Madi et al.3 state that ventricular septal and atrial septal defects are present in 100% and 53% of cases with this disorder, respectively, while tetralogy of Fallot and ventricular diverticula are found in 20% each 3.
This is a rare disorder considering that only about 250 cases have been reported worldwide 4. Thus, it is a rare syndrome with an estimated incidence that varies from 1 cases per 65 000 to 200 000 live births in the different reported series 5-7. Its spectrum is variable and depends on the five basic defects that define it: a midline supraumbilical abdominal wall defect, defect of the lower sternum, defect of the anterior diaphragm, defect in the pericardium, and intra-cardiac defects 8.
As described by Mãrginean et al.9, pentalogy of Cantrell was classified by Toyama 10 into three classes according to the number of defects in each patient. Class 1 or definitive diagnosis has all 5 defects; class 2 or probable diagnosis involves 4 defects; and class 3 or incomplete expression comprises 3 defects.
Pentalogy of Cantrell or thoracoabdominal syndrome is characterized by the variable association of midline body defects with thoracoabdominal wall defects and its differential diagnosis is limb-body wall complex. Both conditions are of unknown cause and early origin but can be explained by an abnormal mesoderm development 11.
The available literature on pentalogy of Cantrell is scarce, mainly because it is a rare disease with great variability in its signs and symptoms of presentation. Reports on this subject are therefore a valuable resource, as they can serve as a basis for future research 12.
Periodic obstetric ultrasound is recommended to detect and treat fetal anomalies since it allows providing optimal perinatal care, considering that approximately half of structural anomalies can be detected in the first trimester. Some of anomalies include anencephaly, abdominal wall defects, holoprosencephaly, and cystic hygromas. However, due to the stages of embryonic development of some organs, it should be kept in mind that certain anomalies are observed at a later gestational age. Similarly, it is worth noting that, as stated by Saldarriaga-Gil et al.13, the second trimester is the best stage for study to identify fetal structural anomalies.
The following is a case of pentalogy of Cantrell associated with craniofacial, limb and reproductive system defects, which was suspected by ultrasound at week 19 of gestation and confirmed postmortem. This is the seventh case of this anomaly reported in Colombia in the last 10 years and the second case in a female patient 8,9,14-17.
CASE PRESENTATION
Stillbirth of 25.2 weeks in whom multiple malformations were identified at 19 weeks of gestation via obstetric ultrasound, leading to the suspicion of a diagnosis of pentalogy of Cantrell. The mother was a 14-year-old mestizo girl from the rural area of La Sierra, department of Cauca, Colombia. No degree of consanguinity with the father was determined, but it was established that this was the mother's first pregnancy.
The first antenatal check-up was carried out in September 2019, when the mother was 19.4 weeks pregnant, and the laboratory tests ordered at that time showed the following results: negative hepatitis B surface antigen; negative IgG and IgM toxoplasma antibodies; positive IgG and negative IgM antibodies against rubella; and positive IgG and negative IgM antibodies against cytomegalovirus. During this first check-up, an ultrasound was also performed, showing a fetus with anencephaly, ectopia cordis, hypoplastic left heart syndrome, diaphragmatic hernia, hyperlordosis, and equinovarus deformity in the right foot (findings compatible with pentalogy of Cantrell). Thus, counseling on voluntary termination of pregnancy was performed due to the severe malformations in the fetus and the risks and future complications; however, the mother preferred to continue with the pregnancy.
At 25.2 weeks of gestation, the mother was admitted to the emergency department of the Hospital Universitario San José de Popayán Empresa Social del Estado due to an 8-hour history of colicky abdominal pain in the hypogastrium accompanied by moderate vaginal bleeding and absence of fetal movements. Obstetric ultrasound was performed, which confirmed fetal death, so labor was induced.
A dead fetus was obtained after delivery, which was sent to the pathology service, where a female stillbirth with height of 23cm, weight of 555g and external malformations was identified. External malformations included amniotic bands attached to occiput and placenta; exencephaly; asymmetric, separated nostrils with ipsilateral nostril and hypoplastic nasal wings, suggesting arrested facial development; broad and flattened nasal bridge; cleft palate; low-set ears; short neck; hypoplasia of the right upper limb; right ectrodactyly; hypoplasia of the right side of the thoracic cage; gastroschisis; ventral hernia with liver content; equinovarus foot deformity; scoliosis with curvature of the spine to the right; and left ovary agenesis (Figures 1, 2, 3). The morphological detail of the images highlights the midline deviation in the face (Figure 1).
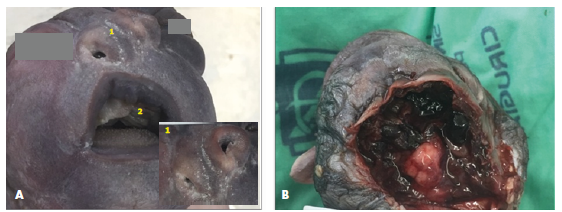
Source: Photographs obtained during the study.
Figure 1 Photographic record of the head of the stillbirth. A) face (1. asymmetric and separated nostrils with ipsilateral hypoplasia of the nostril and nasal wings; and 2. cleft palate); B) medial parieto-occipital region (amniotic band).
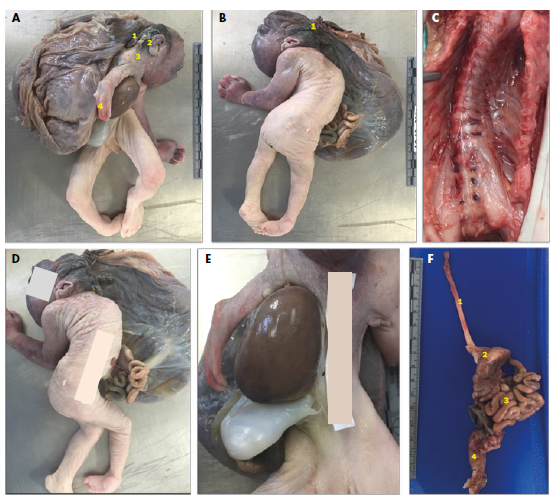
Source: Photographs obtained during the study.
Figure 2 Photographic record of body defects of the stillbirth. A) right lateral view (1. amniotic bands attached to occiput and placenta, 2. low-set ears, 3. short neck, and 4. hypoplasia of the right upper limb ); B) left posterolateral view; C) anterior spinal dissection; D) right lateral view (gastroschisis); E) anterior view (liver outside the body and gastroschisis); F) dissection of the intestinal tract (1. esophagus, 2. stomach, 3. small intestine, and 4. rectum).
During the internal examination of the fetus, it was noted that hypoplasia of the thoracic cage was predominant with asymmetry on the right side and that the diaphragm separated the thoracoabdominal region, although it was displaced to the right and attached to the Glisson's capsule in the right lobe. It was also found that the liver protruded from the abdominal wall and that the area below the thoracic cage was adjacent to the psoas muscles, which were fused. The lungs weighed 3.5g and their overall size was reduced. The short inferior vena cava showed no intracardiac defects (Figures 3, 4, 5 and 6).
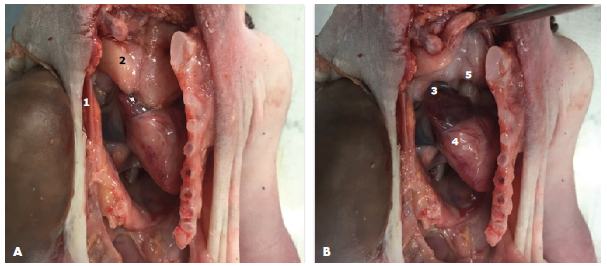
Source: Photographs obtained during the study.
Figure 3 Thoracic cavity dissection. 1) hypoplasia on the right side of the thoracic cage; 2) thymus; 3) right atrium; 4) right ventricle; 5) normal arrangement of the main vessels.
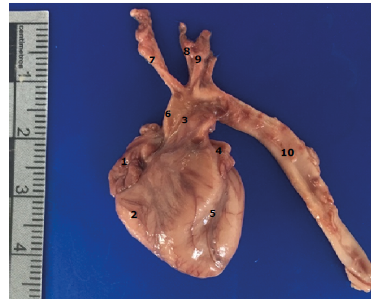
Source: Photographs obtained during the study.
Figure 4 Heart and great vessels. 1) right atrium; 2) right ventricle; 3) pulmonary artery; 4) left atrium; 5) left ventricle; 6) ascending aorta; 7) brachiocephalic trunk; 8) left common carotid artery; 9) left subclavian artery; 10) descending aorta.

Source: Photographs obtained during the study.
Figure 5 Viscera. 1) posterior aspect of the heart; 2) diaphragm; 3) inferior vena cava; 4) left liver lobe.
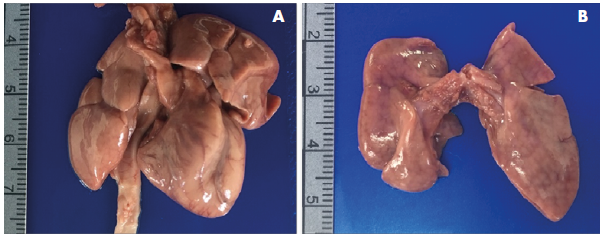
Source: Photographs obtained during the study.
Figure 6 A) Right and left lungs, heart and great vessels; B) lungs.
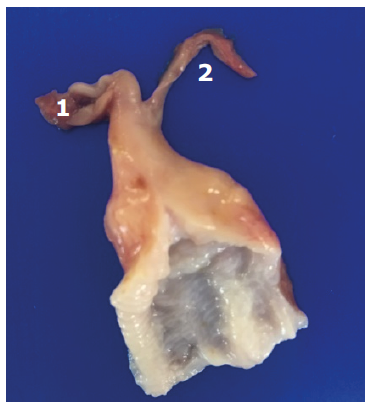
It was also evident that the reproductive system of the fetus was not fully formed and consisted of a uterus, right ovary and fallopian tubes hypoplasia, and agenesis of the left ovary (Figure 7).
Source: Photographs obtained during the study.
Figure 7 Uterus. 1) right ovary; 2) left fallopian tube.
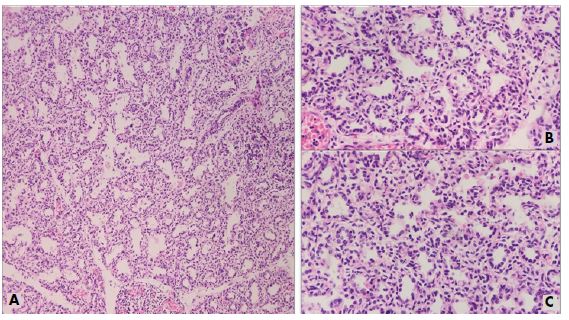
The histology of the organs showed that in the lung parenchyma there was a bilateral, but predominantly right, decrease in the alveolar surface area, with hypertrophy of the tunica media (Figure 8).
Source: Photographs obtained during the study.
Figure 8 Hematoxylin and eosin staining of the right lung. A) 10X view; B) and C) 40X views.
Microscopic examination of the placenta revealed 30% of tertiary chorionic villi with hyalinization, amniotic bands, chronic villitis, chorioamnionitis, and chronic deciduitis with microabscesses.
All the findings described here are part of the spectrum of partial expression or class 2 presentation of pentalogy of Cantrell 9,10, a syndrome suspected based on ultrasound findings and confirmed postmortem. The presence of craniofacial, musculoskeletal and reproductive system defects in the fetus also confirms the diagnosis, as they are described in the literature as additional and rare manifestations of this genetic anomaly 9,18,19.
DISCUSSION
Pentalogy of Cantrell is a poorly described syndrome, but it has characteristic findings that allow to establish its diagnosis. Such findings comprise five basic defects: a midline supraumbilical abdominal wall, defect of the lower sternum, defect of the anterior diaphragm, defect in the pericardium, and intra-cardiac defects 19,20.
Embryological mechanisms involved in the development of pentalogy of Cantrell include abnormal mesoderm development (diaphragmatic, pericardial, and cardiac defects) and failure of fusion of lateral folds (sternal and abdominal wall defect) with changes in the development of a segment of the lateral plate mesoderm between 14 and 18 days of gestation. This leads to failure of the septum transversum to develop and failure of the somatic layer of the lateral plate mesoderm to migrate toward the midline, leaving the thoracoabdominal organs exposed 21.
Pentalogy of Cantrell is also characterized by damage to the amnion that may produce fiber-like bands that limit the development of the fetus, causing constriction on already formed structures 16,17. In the present case, a sternal defect with hypoplasia of the right side of the thoracic cage and thoracoabdominal midline defects, such as gastroschisis and liver eventration, were observed. Likewise, it was established that the fetus had ectopia cordis, although no pericardium defects or intracardiac anomalies were found, which does not rule out the diagnosis of pentalogy of Cantrell 10 because it has been proposed that this disorder has a wide spectrum of presentation, and its characteristics depend on the stage of development in which the defects occur 4.
Some of the causes described for pentalogy of Cantrell include aneuploidies such as trisomies 13 and 18; viral infections; mother's intake of teratogenic agents such as thalidomide, warfarin, and quinidine; vitamin A deficiency in the mother during pregnancy; and some type of familial tendency, with an X-linked dominant inheritance pattern and alteration of the region Xq25-Xq26,l, which is a characteristic of thoracoabdominal syndrome 8,15. However, no association with factors predisposing to malformations was evident in the present case. It should be noted that the patient did not undergo karyotype testing because the mother was young and reported no medical, pharmacological or intoxication history.
Pentalogy of Cantrell is more prevalent in men, with a 1.35:1 ratio 22,23, so this case is of great interest.
One of the described causes of pentalogy of Cantrell is amniotic rupture in cases of ectopia cordis 9, which was evidenced in the case reported here.
Routine ultrasounds performed during antenatal checkups (between 12 and 14 weeks and 19 to 24 weeks of gestation) are extremely helpful in diagnosing pentalogy of Cantrell 19,24. When this disease is suspected in the first trimester of gestation, it may be necessary to carry out complementary studies such as fetal echocardiogram, magnetic resonance imaging and biopsy of the chorial villi, which allows for G- or Q-banding karyotype testing. Such studies are essential, as they allow the identification of the full spectrum of disease presentation and offer the best advice regarding prognosis and follow-up 25. Moreover, early detection of congenital defects allows to offer interdisciplinary support from the beginning of pregnancy, as well as assistance in decision-making about anomalies incompatible with life.
Finally, it is important to mention that during autopsies it is essential to make a detailed macroscopic and microscopic documentation of the findings, that is, a complete record of the malformations of the body must be made so that this, together with the pathologist's report, allows to establish the diagnosis that caused the death. In the present case, the findings corroborated at the autopsy highlight the importance of performing this procedure in cases of multiple congenital anomalies, as it allows the family and even the scientific community to learn about the complications that led to the termination of a pregnancy 26-28.
CONCLUSIONS
Adequate antenatal care, including strict ultrasound follow-up, is essential to detect future complications in the fetus, as well as to provide advice on possible malformations incompatible with life, such as pentalogy of Cantrell, and to determine the best therapeutic approach. Furthermore, autopsies on fetuses with multiple congenital anomalies are indispensable because, as in this case, they allow for the identification of alterations not detected on ultrasound or external physical examination.

