











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Horseshoe kidney is an anatomical anomaly that occurs in approximately one of every 400-600 cases, mainly in men. It is the most common fusion anomaly, although it is relatively infrequent. The main complications are related to the severity of renal fusion, such as hydronephrosis, infections, lithiasis, abdominal pain, and, in some cases, abdominal masses. The greatest challenge posed by this anatomical variation is in the surgical field, given its multiple morphological and vascular forms1,2.
Description of the clinical case
A cadaver of an unidentified man between 40-45 years of age was received for necropsy. He was subsequently and reliably identified as 39-year-old DRP*.
Upon external examination, we found a groomed, medium build, properly dressed man; his shirt had blood on the front and back. No particular signs such as scars, moles, or tattoos were found.
As signs of violence, we observed an entrance gunshot wound in the midclavicula at the level of the fifth intercostal space, with an exit wound in the infrascapular region of the right side; and an entrance wound in the right temporal region, with an exit wound in the temporal parietal region on the left side.
During the internal examination of the body, and after having performed the evisceration of the abdominal pelvic thoracic block, the posterior side was clear, and we found what is called a horseshoe kidney at the abdominal level.
In a macroscopic inspection, without dissecting the kidneys, it was observed that they were connected by the upper poles that are in front of the abdominal aorta artery. Apparently, it did not cause any vascular alteration at the level of the celiac trunk.
The measurements of the anatomical specimen described were as follows:
- The right kidney had a length of 15 cm to the upper pole, where the anastomosis of the two kidneys was located. Its circumference was 11 cm at the level of the renal ileum.
- The left kidney had a length of 16 cm to the upper pole, where the anastomosis of the two kidneys was located. Its circumference was 10 cm at the level of the renal ileum.
Then the course of the ureters was checked, from the renal ileum to the bladder. No double collecting system was found. However, it was described that each kidney had its respective ureter coming from their ileum.
At the vascular level, it can be said that the renal arteries were in their usual position, that is, each one originated from the abdominal aorta. However, it is striking that the site where the kidneys were connected (by the upper poles) had an accessory artery, originating from the abdominal aorta on its dorsal side. This indicates that, in this case, the kidneys did not have two, but three arteries to nourish the entire vascular component of this anatomical variant.
In the venous system we found that, in the upper renal poles (where the anastomosis was located), two veins accompanying the accessory artery were present as an anatomical variant. These veins did not drain into the vena cava but anastomosed almost immediately after exiting the accessory ileum and drained into the renal vein on the right side.
The adrenal glands were in the usual position, as follows:
- The right adrenal gland was attached to the underside of the right lobe of the liver and in relation to the upper pole.
- The left adrenal gland was in its terminal third in relation to the upper pole and over the renal ileum on the same side. It should be noted that, although the anatomical disposition was normal, the gland was much closer to the ileum than usual.
Information about his medical record was requested, with the informed consent of his relatives. After reviewing the entire medical record, no description or test was found that allowed to know that the deceased had this anatomical variant. It is noteworthy that, in the review of the medical record, it was found that the patient consulted, on several occasions, for recurrent urinary tract infections, which resolved with usual antibiotic treatment. In the paraclinical tests of renal function, no abnormality was found, and creatinine levels were as expected for his age; the urine cytochemistry did not show any abnormality.
While alive, his blood pressure was slightly high, without indication of pharmacological management. Only changes in lifestyle were prescribed.
After completing the necropsy, the findings allowed us to conclude that the death of the person who lived under the name of DRP (39) was due to:
Discussion
Normal anatomy of the kidney
The kidneys are approximately 10 cm long, 5 cm wide, and 2.5 cm thick. They are located retroperitoneally in the posterior wall of the abdomen, one on each side of the vertebral column, at the level of the T12-L3 vertebrae. Superiorly, the posterior sides of the kidneys are related to the diaphragm, which separates them from the pleural cavities and the twelfth pair of ribs3.
The superomedial side of each kidney is in contact with an adrenal gland, which acts as part of the endocrine system. The upper urinary organs (kidneys and ureters), their vessels and the adrenal glands are retroperitoneal structures. The renal hilum is at the concave medial edge of each kidney, entering the renal sinus. Structures such as vessels and nerves, and structures that drain the urine from the kidneys, cross the renal sinus through the renal hilum. Posteriorly, the upper portions of the kidneys are located deep with respect to ribs 11 and 123.
In the hilum, the renal vein is anterior to the renal artery, which in turn is anterior to the renal pelvis. Within the kidney, the renal sinus is occupied by the pelvis, calyces, vessels, and renal nerves. The renal pelvis is the flattened, funnel-shaped expansion of the upper end of the ureter. The vertex of the renal pelvis continues with the ureter. The renal pelvis receives two or three major calyces, each of which is divided into two or three minor calyces. Each minor calyx is formed by a renal papilla, the apex of the renal pyramid from which urine is excreted3.
Ureters
They are muscular conduits whose length is 25-30 cm, with a narrow lumen, that transport the urine from the kidneys to the urinary bladder. The ureters run inferiorly from the vertices of the renal pelvis in the hila of the kidneys, and pass over the terminal line at the level of the bifurcation of the common iliac arteries. Then, they run along the lateral wall of the pelvis and enter the urinary bladder. The abdominal portions of the ureters adhere closely to the parietal peritoneum and are retroperitoneal along their course3.
Adrenal glands
They are located between the superomedial side of the kidneys and the diaphragm. They are surrounded by the renal fascia, by which the crura of the diaphragm are connected. They are separated from the kidneys by a thin partition3,4.
The shape and relationships of the adrenal glands differ on both sides. The right gland, pyramidal in shape, is more apical than the left kidney, is located anterolateral to the diaphragm, and is anteromedially in contact with the inferior vena cava and anterolaterally with the liver. The left gland, semilunar in shape, is medial to the upper half of the left kidney and is related to the spleen, stomach, pancreas and left crus of the diaphragm. Each adrenal gland has a hilum through which the veins and lymphatic vessels leave the gland, while arteries and nerves enter it through various points3,4.
The adrenal glands have two parts: the cortex and the medulla. The cortex secretes steroids and androgens. These allow the kidney to retain sodium and water in response to stress, increasing blood volume and pressure. The adrenal medulla is a mass of nervous tissue invaded by capillaries and sinusoids. It is formed by chromaffin cells that secrete catecholamines, especially adrenaline, into the bloodstream in response to stimuli from presynaptic neurons3,4.
Vessels and nerves of the kidneys, ureters, and adrenal glands
The right renal artery passes posteriorly to the inferior vena cava. Each artery is divided near the hilum into five segmental arteries. These are terminal arteries, that is, they do not anastomose with other segmental arteries. The segmental arteries are distributed to the segments of the kidney, as follows:
The upper (apical) segment is irrigated by the superior (apical) segmental artery; the anterosuperior and anteroinferior segments are irrigated by the anterosuperior and anteroinferior segmental arteries; the lower segment is irrigated by the inferior segmental artery. These arteries originate in the anterior branch of the renal artery.
The posterior segmental artery originates in an extension of the posterior branch of the renal artery and supplies the posterior segment of the kidney3.
The renal veins drain the kidneys and connect variably to form the right and left renal veins.
Arterial irrigation and venous drainage of ureters
Arterial branches are born from the renal arteries for the abdominal portion of the ureter, and there are other less constant branches of the testicular or ovarian artery, the abdominal aorta, and the common iliac arteries. The veins draining the abdominal portion of the ureters drain into the renal and gonadal veins3.
Adrenal arteries and veins
The adrenal arteries come from three sources:
Nerves of the kidneys, ureters, and adrenal glands
The nerves of the kidneys come from the renal plexus and are formed by sympathetic and parasympathetic fibers. The renal plexus receives fibers from the abdominopelvic splanchnic nerves. The nerves of the abdominal portion of the ureters come from the renal, aortic abdominal, and superior hypogastric plexus.
The rich innervation of the adrenal glands comes from the celiac plexus and the abdominopelvic splanchnic nerves3.
Horseshoe kidney
The kidney presents different anatomical variations, as described by Watson and Harper, such as pelvic kidney, ectopic crossed kidney, renal agenesis, and horseshoe kidney. It can also have vascular variations such as multiple arteries, overlap of the right renal artery passing over the vena cava, retro-aortic left renal vein, among others4.
The horseshoe kidney is one of the most common anatomical anomalies and refers to the lateral fusion of the kidneys. It is more common in men, and the isthmus can be formed by a fibrous band or functional parenchyma5,6,7.
There are several ways to classify the horseshoe kidney: by its macroscopic form and fusion site, its clinical picture, or its vascular distribution.
According to the place where the fusion occurs:
"U" horseshoe kidney shows medial fusion and is located symmetrically on both sides of the spine.
"L" horseshoe kidney results from the lateral fusion between a horizontal and a vertical kidney, and the lateral isthmus is located towards the midline5.
The horseshoe kidney may be at any height of the normal course expected from the rise of the kidneys, but they are mainly found in the lower portion of the lumbar spine. This is due to the restricted rise at the level of the origin of the inferior mesenteric artery, approximately between L3 and L5, and anterior to the abdominal aorta and the inferior vena cava. The ureters usually pass through the anterior section of the fused poles and descend medially. They may have arterial supply from the iliac, sacral, mesenteric, or aortic arteries5,6,7 (Figure 1).
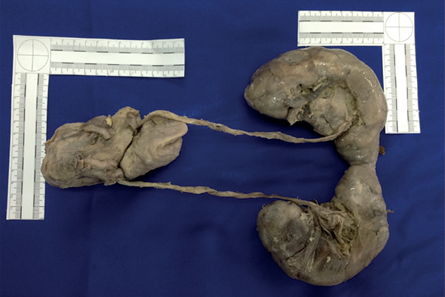
Figure 1 View of the complete specimen of horseshoe kidney with urinary tract, bladder, and prostate.
Clinically, it can be classified into three groups:
Present anomaly, but without pathological changes or symptoms. There is no hydronephrosis or complications since the ureteropyelic junction is wide.
Present anomaly without pathological alteration, but the patient complains of symptoms such as abdominal pain, which is caused by compression of the abdominal aorta. There is vascular and nervous compression and multiple urinary disorders such as lithiasis or frequent infections. This anomaly is known as Rovsing syndrome or horseshoe kidney disease. The pain is exacerbated when the person sits after being in a supine position, or when they go from sitting to standing up.
The anomaly occurs with complications. The symptoms are due to pathological conditions. Due to the posterior location of the calyces there is ureteropyelic stricture. There are no individual or group symptoms that indicate specific changes between a horseshoe kidney or a normal one. This anomaly can only be determined by urological diagnostic methods such as excretory urography and retrograde pyelography, CT, sonography, and angiography.
For a better organization, six basic patterns have been established that allow to classify the different types of irrigation:
1a: All segments of the horseshoe kidney are irrigated by a single artery, except collateral circulation, which may have a single renal artery for this function.
1b: The upper and middle segments may have a single renal artery, with a branch of the abdominal aorta for arterial blood supply to the lower segments.
1c: The lower segments are irrigated by arteries that arise from a common trunk, coming from the abdominal aorta, and the upper and middle trunks are irrigated by a renal artery for each side.
1d: The upper and middle segments have irrigation from multiple renal arteries.
1e: The isthmus also has irrigation of arteries that come out below it, usually coming from the abdominal aorta, either independently, or from a common trunk.
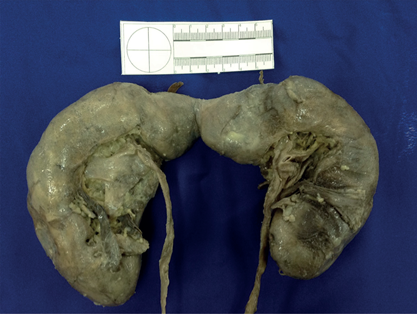
1f: The fused lower segments can have irrigation from the branches of the common iliac artery, or in less common cases, the internal iliac artery or middle sacral artery7,8 (Figure 2).

Figure 2 Anatomical detail of the renal hilum and accessory artery in the lower poles of the kidneys.
It has been reported that the horseshoe kidney is associated with calyceal, ureteral, and vascular abnormalities. It may have normal irrigation of accessory renal arteries, which originate at different levels and enter through the renal hilum, and also aberrant arteries, which directly enter the poles or the isthmus of the kidney. Except for some arteries entering the isthmus, no vessel has been seen entering the kidney by its dorsal side.
The horseshoe kidney is frequently accompanied by anomalies of the inferior vena cava (such as the double, left, or pre-isthmus inferior vena cava), and its coexistence is probably due to its embryonic origin.
The abnormal position of the kidneys together with their shape makes them more susceptible to severe damage after some type of abdominal trauma, since they are not protected by the ribs8.
The horseshoe kidney has symptoms generally attributed to associated anomalies, such as hydronephrosis, infections and lithiasis, although it is almost always asymptomatic. The most observed symptom is abdominal pain, which radiates to the lumbar spine. Urinary tract infections caused by urinary stasis can also occur. Gastrointestinal symptoms such as pain, nausea, and vomiting have been reported. Occasionally, there may be a mass at the abdominal level, which is confirmed by an intravenous pyelogram or ultrasound5,6,7,8 (Figure 3).
Conclusions
The findings allow to determine that the presence of the horseshoe kidney is not so unusual in our environment.
Most people who have a horseshoe kidney are asymptomatic most of their lives.
The renal function tests, in this specific case, do not show alterations outside the usual for the age.
The major complications of the horseshoe kidney lie in the surgical approach, when it is found incidentally, as well as in the excretory function tests and its interpretation with this variant.
It is not clear whether, in this case, the horseshoe kidney is related to the elevation of blood pressure levels.
Contribution of authors
Catalina Vásquez: performed the necropsy protocol. Frank David Rojo: dissected the specimen. Juan David Ríos, Karen Ruiz Naranjo and Carolina Sarmiento: made the literature review. The text was drafted by all members of the group.

