











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
The hypoplasia of renal arteries is a rare disease. It is characterized by hypotrophy of tubular appearance of these arteries; its clinical consequences are derived from the intrarenal hemodynamic repercussions. Despite this, the descriptions in the literature of this disease are limited to some case reports with compromise primarily of the thoracic and abdominal aorta. However, below is described the case of a young patient with a diagnosis of hypoplasia of renal arteries.
The patient has a previous diagnosis of essential arterial hypertension. Upon admission, a picture of exacerbated chronic kidney failure is documented, coupled with high blood pressure readings. Despite ambulatory antihypertensive management, this finding is not explained by the clinical picture by which he consults. Throughout his hospital stay and during the performance of paraclinical studies he is diagnosed with hypoplasia of renal arteries.
Presentation of the clinical case
A male patient of 30 years of age, mestizo, born in Neiva, resident in the city of Popayan, student of Civil Engineering. He has an important antecedent of arterial hypertension, diagnosed in the outpatient clinic two years ago, without complementary studies and managed as essential hypertension with losartan 50 mg every twelve hours, without other relevant data. The patient has a history of rhinoplasty due to a previous trauma ten years ago. He does not refer any other pathological antecedent.
The patient enters to the outpatient service in the San Jose University Hospital, due a clinical picture of fifteen days of evolution, consisting in non-dysenteric diarrheal stools, associated with episodes of emesis of food content, without abdominal pain, dysthermias or another type of symptomatology. In the admission physical examination, it was found that the patient was in fairgeneral conditions and had the following vital signs: blood pressure of 140/78 mmHg, heart rate of 102 beats per minute, 21 breaths per minute and temperature of 37° C. In the general inspection, stands out the marked conjunctival pallor and jugular ingurgitation at 30°; at the pulmonary level, fine crackles in both bases of the lungs without additional abnormal sounds; grade II edema was documented at the level of the lower limbs. No other positive finding was evidenced. It should be clarified, anyway, that a thorough clinical examination was carried out.
On admission, paraclinical tests were requested, in which stood out markedly elevated levels of nitrogen compounds with electrolyte alteration, given by the presence of hyperkalemia without electrocardiographic repercussion and normocytic normochromic anemic syndrome. Hyposthenuria, proteinuria, hematuria and granular casts were evidenced by means of a urine test (Table 1).
Table 1 Paraclinical tests at admission and discharge
| Laboratory test | Admission | Discharge | Interpretation |
| Leukocytes | 9,300 cells/mm3 | 7,800 cells/mm3 | Without changes: normal |
| Neutrophils | 7998 cells/mm3 | 5928 cells/mm3 | Without changes: normal |
| Lymphocytes | 744 cells/mm3 | 1248 cells/mm3 | Without changes: normal |
| Hemoglobin | 12.1g/dL | 13.2 | Low |
| Hematocrit | 36.9 % | 38.7% | Low |
| Platelets | 182,000 x 103/mm3 | 184,000 103/mm3 | Without changes: normal |
| Prothrombin time | 10.1 s. | 9.7 s. | Without changes: normal |
| Partial Thromboplastin time | 27 s | 26 s. | Without changes: normal |
| C-reactive protein | 1.1 mg/dL | - | Negative |
| Serum Creatinine | 10 mg/dL | 7.8 mg/dL | Elevated |
| Serum urea nitrogen | 69 mg/dL | 38 mg/dL | Elevated |
| Sodium | 134 mEq/L | 139 mEq/L | Normal |
| Potassium | 6.6 mEq/L | 3.7 mEq/L | Hyperkalemia with subsequent normal potassium |
| Serum lactate | 1.8 | - | Normal |
| 24-hours proteinuria | 1712 mg/24hours | - | Non-nephrotic range proteinuria present |
| Complement factors C3-C4 | 160 and 37mg/dl | - | Normal |
| Antinuclear antibodies (ANAs) | Negative | - | Negative |
| Anti-DNA antibodies | Negative | - | Negative |
| Antineutrophil cytoplasmic antibodies (ANCA IgG) | Not detected | - | Negative |
| Perinuclear fluorescence pattern (P-ANCA) -cytoplasmic (C-ANCA) | Not detected | - | Negative |
| Antithrombin III | - | 70 - 130 % of inhibition | |
| Protein C | 98 % | - | 60 - 150 % of inhibition |
| Protein S | 118 % | - | 60 - 150 % of inhibition |
| Leiden Factor V | Negative | - | Negative |
| Urine citochemistry | PH:6, Proteins: lOOmgdl Density: 1,005 Glucose: {-) Casts: {-) Bilirubins: {-) Urobilinogen: {-) Nitrites: (-) Hemoglobin: SO Leukocytes: 0-2 XC Redblood cells: 6-8 XC Epithelial ceEs: 0-1XC Bacteria: Scarce Granular casts: IXC | Altered: proteinuria-hyposthenuria-hematuria granular casts |
Taking into account the lack of previous studies and the antecedent of hypertension, previously classified as essential, it was suggested that, at the moment, the patient hadan exacerbated chronic kidney disease of pre-renal origin AKI-III secondary to his diarrheal disorder. However, in view of the age and the paraclinical tests on admission, other pathologies were taken into consideration. Therefore, syndromic treatment was started with amlodipine, controlled liquids scheme and measures to control hyperkalemia, such as terbutaline nebulizations, furosemide, calcium gluconate and ion exchange resins.
Despite the management established, the patient did not show a satisfactory clinical evolution, since he presented subsequent onset of anuria, hypervolemic status, metabolic acidosis, persistence of hyperkalemia without electrocardiographic changes and blood pressure readings with tendency to elevation. For this reason, he was evaluated by the nephrology service which initiated renal replacement therapy 48 hours after admission, with improvement of the uremic status and hypervolemia.
Subsequently, it was requested a renal ultrasonography with Doppler of renal arteries, which documented as an important finding: kidneys with reduced dimensions, presence of symmetric bilateral renal atrophy with increased echogenicity, compatible with chronic nephropathy without dilation of the collecting system, masses or calculi.
The study reported that the left intrarenal vessels, both arterial and venous, had a normal appearance, but it was not possible to visualize the right vessels.
Next, it was requested an immunological profile and other acute phase reactants that resulted negative. For this reason, the nephrology group of the hospital decided to carry out a renal arteriography, given that angioresonance was not available at the time, after stabilization of his hydroelectrolytic and azotic status, with a protocol of nephroprotection protocol and subsequent hemodialysis. This study determined the presence of hypoplasia of renal arteries (see Figures 1 and 2).
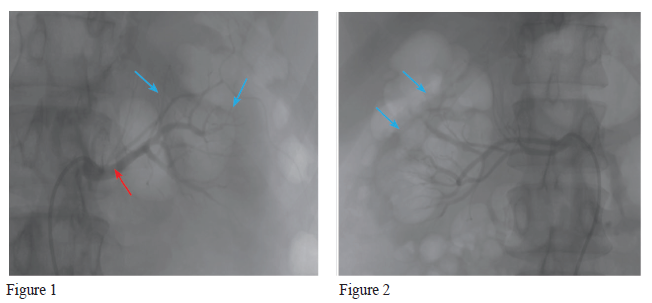
Figures 1 and 2 Renal arteriography. The right and left renal arteries are of small caliber with bifurcation in the proximal and medial third, almost ostial, with polar arteries of very small caliber (blue arrows), being visualized in the delayed nephrographic phase (red arrow), without the presence of aneurysmal dilatations, other obstructions or arteriovenous malformations.
Finally, it was defined a discharge plan for the patient, given the clinical and paraclinical improvement in the status of exacerbation of his renal failure, with a diagnosis of renal artery hypoplasia. Consequently, an external management plan was given with amlodipine 10 mg day and clonidine 150 mcg every twelve hours, with general recommendations and strict ambulatory control for follow-up by nephrology, extension studies and evaluation of the need for renal replacement therapy.
Discussion
Renal artery hypoplasia continues to be a confusing clinical problem, due to the low prevalence of this condition. This has restricted the development of a specific definition and an adequate clinical approach. The pathology is part of a large number of conditions included in the CAKUT (congenital anomalies of the kidney and urinary tract) syndromes, and it is characterized by a subnormal growth of the kidney that compromises, in turn, the renal artery and its branches, which are, in addition, hypoplastic and usually sclerotic.1
The term congenital renal hypoplasia indicates the presence of a child-sized kidney with a preserved excretory function, in contrast with the functional alterations related to vascular malformations characteristic of renal artery hypoplasia.2 Thus, the hypoplasia of an artery is defined as a regular, elongated and tubular narrowing of the segments of such structure.3 Although its pathophysiology is not clearly known, both congenital renal hypoplasia and hypoplasia of renal arteries have a common pathophysiology, related to defects in embryogenesis, which include alterations in the development of the nephrogenic blastema of metanephrogenic ducts or primary vascular deficiencies.
The main manifestation of hypoplastic and stenotic arteries is the appearance of renovascular hypertension. This situation can be explained through the phenomenon described by Goldblatt, in which, in animal models with only one kidney, the occlusion of one of the three main branches of the renal arteries resulted in a significant increase in the levels of renin and appearance of secondary arterial hypertension.4-5
As it has been mentioned, regarding the frequency of this condition, it should be noted that, as it is an unusual pathology, there are few reports of adult patients in the literature2 and, generally, it is diagnosed in the first stages of life, with different latency periods.3-7
Therefore, it is not uncommon to find an association between renal artery hypoplasia concomitant with aortic hypoplasia and a variable frequency between 33% and 81%.3 However, both conditions are extremely rare and unusual.8 As previously stated, this pathology may debut clinically with acute renal deterioration or appear as an hypertension picture of difficult management in young patients. Therefore, although it is infrequent, it should be suspected in patients with characteristics such as those mentioned above.
Considering the above, the availability of paraclinical tests and diagnostic images that allow an adequate approach and does not delay the diagnosis of this pathology is of vital importance. For this reason, arteriography is the study of choice, since it allows to define whether the hypoplasia is congenital or is a case of renal atrophy, taking into account that, in hypoplasia, the renal artery is present, although with a smaller size and length, as defined by Love et al.9 Frequently, the most prominent angiographic features of this pathology consist in the presence of a renal artery of a smaller size from its origin to the bifurcation, which implies a narrowing with tubular contours without focal stenoses.
Likewise, the lobar and arcuate arteries are bifurcated adequately, but are smaller,2 unlike renal atrophy, in which the size of the artery is diminished in its origin, but its branches have an irregular appearance in their different segments with focal stenoses.
Finally, it is important to stress that, among the management strategies for this condition, there are no clinical guidelines or meta-analyzes. This circumstance can be attributed to the scarce literature available, so that its therapeutic approach should be based on the patient's clinical condition and on the degree of organic involvement. Nephrectomy is an option in those cases where the commitment is unilateral and good outcomes are obtained in objectives such as controlling the blood pressure readings and avoiding the commitment of other target organs due to arterial hypertension.6,10
Conclusion
Hypoplasia of renal arteries is a rare disease and should be taken into account in the approach of patients with secondary arterial hypertension. This article emphasizes the importance of comprehensively addressing a patient who debuts with hypertension at an early age and without a family history of hypertension. With this intention, we describe the case of this hypertensive patient without outpatient studies, whose clinical presentation led to us to rule out common causes in our environment. Given that the imaging finding was the key to reaching the diagnosis, the discovery of this pathology, among other causes of secondary hypertension, requires a high index of suspicion, as well as the availability of diagnostic support with images (angioresonance or arteriography, as in this case), to prevent further complications related to sustained blood pressure elevations.
Ethical responsibilities Protection of people and animals
The authors declare that no experiments were performed on human beings or animals for this research.
Data confidentiality
The authors declare that they have followed the protocols of their workplace on the publication of patient data.
Right to privacy and informed consent
The authors state that patient data do not appear in this article.

