











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Executive functions (EF) are higher-order cognitive processes associated with processing in the prefrontal areas of the brain [1] responsible for efficiently guiding goal-directed behavior. EFs allow the subject to plan, monitor, evaluate performance, adapt to new situations, and solve complex problems in which there has been no prior learning [2]. In general, EFs are cognitive processes that guide, coordinate, review, and evaluate behavior in achieving goals [3,4].
Currently, there is no consensus on the definition and classification of EF; therefore, the evaluation and training approach depends on the theoretical models that support them. One of the most recognized models has been the proposal by Miyake et al. [5], who, through a confirmatory factorial analysis, defined working memory, cognitive flexibility, and inhibitory control as central nuclei of executive functions, cognitive processes from which others of greater complexity would derive, such as reasoning, problem-solving problems, and planning. Other theoretical models include others (EF), such as verbal fluency [6], planning [7], decision-making [8], and some attentional control processes [9].
Beyond explanatory theoretical models, it is a reality that Executive Functions can present impairment in various clinical pictures, such as syndromes associated with damage to the prefrontal cortex, especially in the dorsolateral, medial, and orbitofrontal areas; the involvement of each one of these areas is expressed in clinical pictures with different alterations of executive functioning [10,11].
EF impact is a characteristic of a large number of health disorders in young and middle adults with some early-onset neurodegenerative disorders, neurodevelopmental disorders (e.g., autism, attention deficit disorder, and intellectual disability), mood disorders, psychoactive substance use disorders, obsessive-compulsive disorder, stroke, genetic disorders such as Huntington's disease and Gilles de la Tourette syndrome, as well as other diseases such as cancer and HIV [12].
Among the processes of cognitive intervention for the clinical population and the healthy population, the rehabilitation or stimulation paradigms can be recognized. The first focuses on cognitive processes affected by the disease, injury, or neurodegenerative condition. Stimulation, on the other hand, provides opportunities for developing and promoting the capacities of cognitive processes that have not yet been consolidated. In other words, while rehabilitation is based on the principles of restitution, compensation, and substitution, stimulation is based on the principles of transference and generalization [12,13].
Concerning these programs, the literature suggests that intervention schemes should be aimed at improving cognitive processes and their neurological bases under the principle of neuroplasticity, producing a reorganization in brain structure and functioning [12]. The studies also propose that the activities of said programs should aim at processes rather than task training, so that in addition to generating close transfer, associated with improvement in untrained tasks that measure the same cognitive component, they also succeed in causing a far transfer, that is, an improvement in untrained tasks that measure related cognitive components [14].
One of the alternatives for rehabilitation and cognitive stimulation has been programs based on computer systems. Studies on this type of program have shown a promising panorama in different age groups. However, some of the findings restrict their effectiveness to early ages or older adults; other studies position these technologies among the new directions of cognitive training, with effects throughout life, albeit with varying degrees of efficiency [15-18]. For this reason, research evaluating the feasibility and effects of computerized cognitive training programs remains a growing need in a way that allows exposing the feasibility of incorporating these programs into clinical practice [15,19].
Reviews that evaluate the effectiveness of computerized cognitive training programs on executive functions in different population groups have shown contradictory results, to a certain extent associated with characteristic methodologies of these studies [20]; most of these reviews have focused on the elderly [21,22] with sequelae of cerebrovascular accident [23], and adults with cognitive impairment. These studies have found improvements in general cognitive function in older adults [21]; however, the effect on executive functions has not been studied. Only one review was conducted on the average adult [24]; the authors restricted the search to interventions with more than 12 weeks and found only one article with eligibility criteria. In their work, they concluded that computerized cognitive training in midlife demonstrated lasting effects on general cognitive function with 12 weeks of training and memory after 24 weeks of training [24].
Based on this background and in the absence of reviews on the topic of interest, it is proposed to carry out a scoping review with the aim of providing a general description of the evidence collected so far on cognitive stimulation and rehabilitation programs for executive functions, based on computer systems applied in young and middle adulthood.
Methods
Protocol and registration
The selected methodology was the scoping review, since it is better suited to the proposed objective, which is to provide a general description of a particular topic to identify knowledge gaps and support new studies [25]. The scoping review is formulated as a stepwise process of five phases: 1) identify the research question; two) Identify relevant studies; 3) select studies; 4) graph the data; and 5) summarize and report the results [26]. The present study's authors formulated an a priori protocol following the PRISMA ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) extension for scoping reviews checklist [27], and it was reviewed by an external peer specialized. Said protocol is not publicly available, but it is available on demand through the correspondence author's email.
Eligibility Criteria
The established inclusion criteria were research articles published between 2015 and 2022, experimental studies (controlled clinical trials, open clinical trials, and quasi-experimental studies), articles that study computerized programs for the stimulation or rehabilitation of executive functions that involved the population between 18 and 60 years of age, written in English, and that included one or two measures of executive functions. The exclusion criteria were established as follows: short articles, summaries or protocols, reviews and meta-analyses, articles that do not evaluate executive functions, interventions that are not based on the use of computer systems, and studies in populations under 18 or over 60 years of age.
Information sources
To identify potentially relevant documents, the following bibliographic databases, resource sources, and digital platforms were searched: Science Direct, Scopus, Springer Link, PubMed, and Taylor & Francis. The research team designed and tested the search strategies and reviewed them with a specialized professional. In the review protocol, the authors established the central concepts for the construction of the search chain of the studies: 1) Executive functions, 2) Rehabilitation and cognitive stimulation, 3) Computer systems, and 4) young and middle adulthood. These categories were translated into English and reviewed in the ERIC thesauri (recognized terms in education and health from the Educational Resources Information Center). Based on these central concepts identified and the review carried out in said thesauri, a search chain was built that included logical operators, which was executed in October 2022 in the databases selected for the search of the articles. The final search strategy for each database is presented in Table 1.
Table 1 Search strategy for each database or digital platform.
| Database (total records) | search algorithm | automatic filters |
|---|---|---|
| Science direct (96) | Year:2015-2022Title, abstract, keywords: (( "Executive function" OR "executive function" OR "Executive functioning") AND ("cognitive training" OR "Cognitive Stimulation" OR rehabilitation ) AND ( computerized OR based-computer ) | -The "Years" filter was applied (2015 to 2022) |
| -The "Type of article" filter was applied by selecting the option "Research articles" * | ||
| Springers (243) | ("Executive function" OR "executive function" OR "Executive functioning ") AND ("cognitive training" OR "Cognitive Stimulation" OR rehabilitation) AND (computerized OR based-computer) | -The "Data published in" filter was applied (2015 and 2022) |
| -The "Type of content" filter was applied, selecting the "Article" option * | ||
| Pubmed (148) | (("Executive function"[Title/Abstract] OR "Executive function" [Title/Abstract] OR "Executive functioning" [Title/Abstract]) AND ("cognitive training" [Title/Abstract] OR "Cognitive Stimulation" [Title /Abstract] OR "rehabilitation" [Title/Abstract]) AND ("computerized" [Title/Abstract] OR "computer-based" [Title/Abstract])) AND (2015:2022[ pdat ]) | -The "Publication date" filter was applied to select works published between 2015 and 2022. |
| -The "Type of article" filter was applied, selecting the options "Clinical trial" and "Randomized controlled trial" * | ||
| Taylor & Francis (184) | [[All: "executive function"] OR [All: "executive function"] OR [All: "executive functioning"]] AND [[All: "cognitive training"] OR [All: "cognitive stimulation"] OR [All: rehabilitation]] AND [[All: computerized] OR [All: computer-based]] AND [Article Type: Article] AND [Publication Date: (01/01/2015 TO 12/31/2022)] | -The "Publication date" filter was applied to select works published between 2015 and 2022. |
| -The “Source type” filter was applied, selecting the option “Scientific journals” and “Theses and doctoral dissertations” * | ||
| Scopus (225) | TITLE-ABS-KEY (("Executive function" OR "executive function" OR "Executive functioning") AND ("cognitive training" OR "Cognitive Stimulation" OR rehabilitation) AND (computerized OR based-computer)) AND PUBYEAR > 2014 AND PUBYEAR < 2023 AND PUBYEAR > 2014 AND PUBYEAR <2023 AND (LIMIT-TO (DOCTYPE, "ar"))) | -The "Year" filter was applied to select documents published between 2015 and 2022. |
| -The "Type of document" filter was applied to select the options "Article" and "Conference article" * |
Note. Excluding from the search results the documents of review articles, meta -analyses, brief reports, editorials, publications, case reports, conference information, book reviews, encyclopedia, brief communications, protocol documents, reference work, conference article , book, encyclopedia and conference proceedings, audio and video works, newspapers, brochures and encyclopedias, reports and bibliographic reviews, case studies, reports, reviews of search results.
Selection process
The first author searched the different databases, implemented automatic filters, and eliminated duplicate articles. Next, the first and second authors screened the title and abstract of each article based on the established inclusion and exclusion criteria. The third author carried out a second review of the articles that had passed the first filters. Subsequently, the full text of each article was reviewed independently by the three authors to verify whether or not the eligibility criteria were met; the articles in doubt were reviewed collectively to reach an agreement between the authors, and, in exceptional cases, they were sent for arbitration to an external adviser.
Data extraction
Based on previous reviews, the authors adapted a documentary analysis matrix in which the data extracted from each article were recorded: identification data, place of publication, year of publication, sample size, mean age of the participants, clinical conditions of participants, methodological design, study objectives, characteristics of the training and type of activities, characteristics of the implemented computer system, executive functions studied, measurement instruments, primary results, secondary results, and conclusions.
Results
Once the search chain was executed, 896 records distributed in the different databases were identified. By applying the automatic filters of the search tool (time range, complete articles, original articles, English language, disciplinary areas of interest) and excluding duplicates, the titles and abstracts were screened to proceed to a review of the full text. After assorting these filters, the articles included for the review and analysis comprised 91 studies (see Figure 1). In Appendix A, you can consult the descriptive matrix in which the main characteristics of each study are summarized.
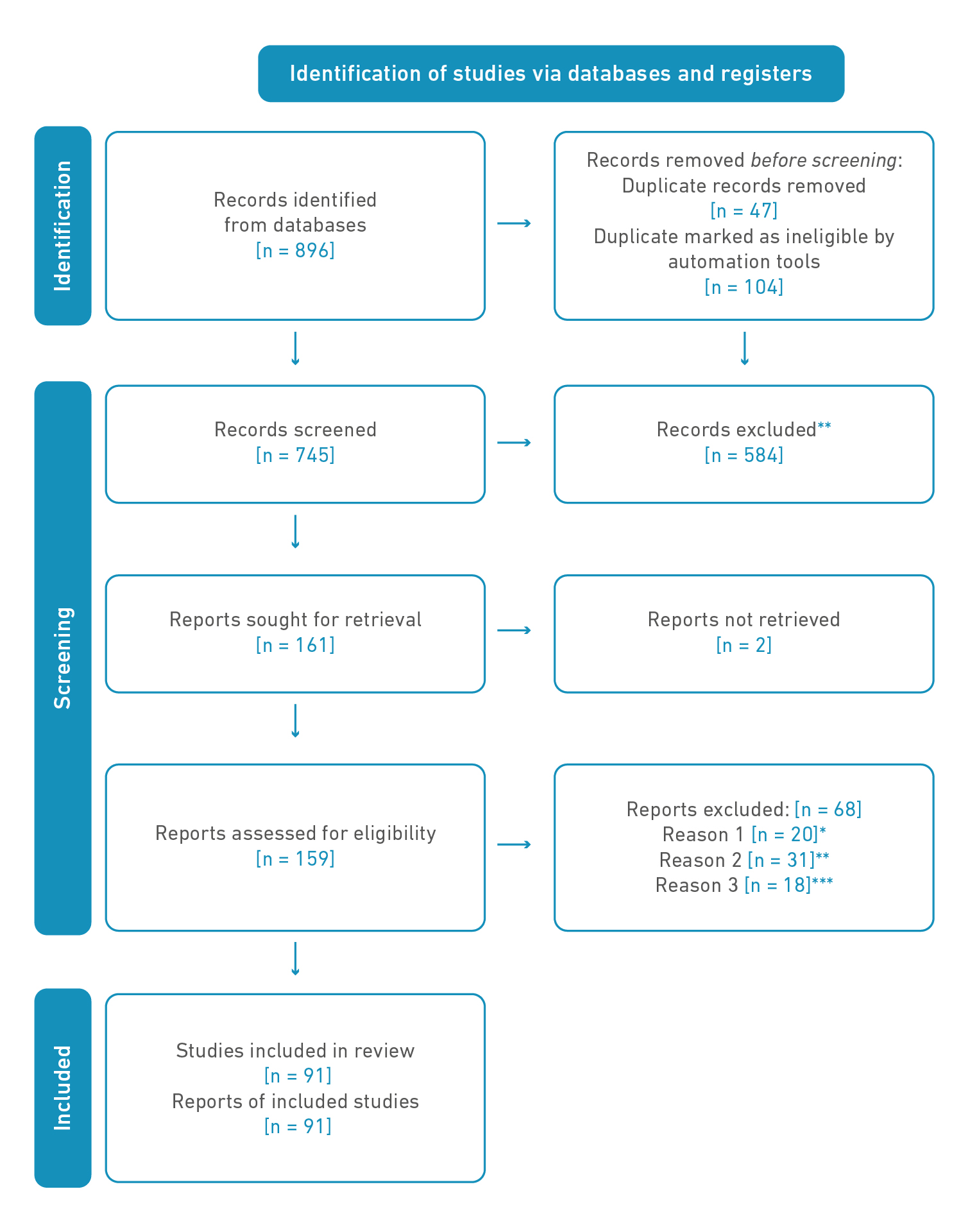
Note 1. * The study did not assess executive functions; ** The population was not young adults or middle adults; *** The intervention was not computerized.
Note 2: Science Direct (96), Scopus (225), Springer Link (243), PubMed (148) and Taylor & Francis (184). When reviewing the title and abstract, it was identified that the articles did not correspond to empirical studies (review articles, opinion articles, short articles, conferences, clinical protocols, posters, they do not present research results), they did not study cognitive training programs based on computer systems or did not investigate in the selected population.
Figure 1. Flowchart
Most of the studies published in the last eight years were developed in North America (34%), followed by Spain (9.1%), Germany (6.8%), the United Kingdom, and Italy (5.6%). Only one of the studies was carried out in a Latin American country (Cuba). Of the total of 88 studies, 32 were in young adults with a mean age of 22.8 years (Standard Deviation 2.4), and 55 were in middle adults with a mean age of 42.9 years (Standard Deviation 9.2).
To present the results, young adults (between 18 and 30 years) and middle-aged adults (between 31 and 60 years) were discriminated against. As seen in Table 2, most of the studies on young adults were conducted in a healthy population, with most of the participants being university students. Most of the clinical population of this population range had a diagnosis of schizophrenia or depressive disorders. The studies in average adults were mainly in the clinical population, where the most frequent pathologies were disorders associated with the schizophrenia spectrum (21.8%) and multiple sclerosis (18.2), to a lesser extent, consumption disorders of substances (10.9%) and cerebrovascular accidents.
Table 2 Clinical characteristics of the study population.
| Characteristics of the study population | Total | Young adult | Middle adult |
|---|---|---|---|
| Frequency (%) | N = 91 | N = 30 | N = 61 |
| Healthy population | 27 (29.7) | 23(76.7) | 4 (6.6) |
| Multiple sclerosis | 13 (14.3) | 13(21,3) | |
| Schizophrenia spectrum | 11 (12.1) | 4 (13.3) | 7 (11.5) |
| Acquired brain damage | 8 (8.7) | 8 (13.1) | |
| Disorders associated with substance use | 8 (8.7) | 1 (3.3) | 7 (11.5) |
| Depressive disorders | 8 (8.7) | 5 (16.7) | 3 (4.9) |
| Attention deficit hyperactivity disorder | 4 (4.4) | ||
| Cancer survivors | 3 (3.3) | 3 (10) | 4 (6.6) |
| Mild cognitive impairment | 3 (3.3) | 3 (4.9) | |
| Anxiety disorders | 3 (3.3) | 3 (4.9) | |
| Human immunodeficiency virus | 2 (2.2) | 2 (3.3) | |
| Huntington's disease | 2 (2.2) | 2 (3.3) | |
| Obsessive compulsive disorder | 1 (1,1) | 1 (1.6) | |
| Chronic fatigue syndrome | 1 (1,1) | 1 (1.6) |
Note: The frequency of the studies is discriminated by young adult and middle adult population, with the respective percentage weighted by population in parentheses.
Regarding the executive functions studied, some of the studies reviewed (24.2%) were based on theoretical models that contemplate the executive function construct in a unified way, making a general reference to the ability to regulate different cognitive, behavioral, and affective functions [28]. In contrast, the rest of the studies assessed executive functions independently.
Similar to the findings of previous systematic reviews conducted in other age groups [29], the most studied executive function was working memory (62.5%), both in clinical and healthy populations. At the same time, some executive cognitive domains were more representative in specific age ranges, such as attention and processing speed, addressed in 58.2% and 38.2% of the studies in middle-aged adults, respectively, but not as a representative in young adults, where most of the studies focused on working memory (69.6%) and, to a lesser extent, attention (18.2%) and inhibitory control (15.1%). Other domains, such as planning and verbal fluency, were studied exclusively in average adults (see Table 3).
Table 3 Executive functions studied by age group.
| Frequency (%) | Total | Young adult | Middle adult |
|---|---|---|---|
| N = 91 | N = 30 | N = 61 | |
| Executive functioning | 31 (33.3) | 7 (20.6) | 24 (39.7) |
| Work memory | 55 (60.4) | 20 (66.7) | 35 (57.1) |
| Attention | 33 (35.4) | 6 (17.6) | 28 (44.4) |
| Cognitive flexibility | 14 (14.6) | 3 (98.8) | 11 (17.5) |
| Inhibitory control | 16 (16.7) | 6 (17.6) | 10 (15.9) |
| Processing speed | 27 (28.1) | 4 (11.7) | 23 (36.5) |
| Planification and organization | 6 (6.3) | 6 (9.5) | |
| Problem resolution | 6 (6.3) | 2 (5.8) | 4 (6.3) |
| Emotional regulation | 6 (6.3) | 2 (5.8) | 4 (6.3) |
| Verbal fluency | 6 (6.3) | 6 (9.5) | |
| Decision making | 4 (4.1) | 2 (5.8) | 2 (3.2) |
Note: The frequency of the studies is discriminated by young adult and middle adult population, with the respective percentage weighted by population in parentheses.
Among the rehabilitation or cognitive stimulation programs based on computer systems, the review allowed us to identify both commercial programs and novel programs designed by the same authors or research groups, with the former used in 60% of the investigations. 52% of the interventions implemented game-based activities, ranging from gamified versions of classic exercises to the design of serious games for specific purposes or commercial video games. 16% of the programs were based on classical tasks, and 4.5% on multimodal programs that included other types of interventions such as physical activity and meditation, in addition to computerized training. The most used device was the computer (57.9%); other devices were tablets (11.3%), smartphones (2.2%), and video game consoles (2.2%), although 26% of the studies did not specify the type of device used.
Most research on young adults was done on healthy people, while most of the research on mid-adults was done on people with clinical conditions. The most representative findings by population group are described below.
Schizophrenia
The most frequent computerized cognitive training program in the studies of the population with the schizophrenia spectrum was the commercial platform Brain HQ, which was included in 7 of the investigations. Studies showed mixed results, some reporting significant effects of training on working memory [30-32], processing speed [30,32-35], attention [32,30], and problem-solving [31], also proving to be a good complement to pharmacological treatment [34]. However, some studies did not find cognitive benefits of the Brain HQ intervention in cognitive functions such as processing speed [36] and the combination with COGPACK [37]; the authors indicate that this lack of effects could be due to the age of the participants (older than in other studies) and that the effects of the medications could reduce the effectiveness of the treatment [37]. However, the same authors report good adherence and satisfaction of the participants towards the treatment.
Among the studies carried out with Brain HQ in the schizophrenia population with comorbid depression and anxiety [32], it was found that a predictor of cognitive gain in working memory and attention is the patient's commitment to treatment, as well as the level of cognitive performance at the beginning of the treatment, finding that those who benefited the most from the training were the people who showed the lowest performance in the pretest. On the other hand [30], she points out that a significant predictor was the number of hours of treatment, such that a greater number of hours of training produced larger improvements in working memory and processing speed. In a study evaluating the combination of Brain HQ training and Modafinium pharmacological treatment, the authors found improvements in trained tasks; however, the medication group showed no differential effects from the group receiving cognitive training alone [34]. Auditory-targeted cognitive training with Brain HQ also showed a positive correlation with measures associated with auditory processing speed in this population [35].
Another of the programs studied in the population with schizophrenia was CIRCuiTS, a computerized program for cognitive remediation. Interventions with this program led to better performance in visual memory [38], working memory, and processing speed [39], but showed no effect on attention, reasoning, and problem-solving. However, it was demonstrated to be a protective factor against cognitive decline in this population [39]. A study with the Neuronpersonaltrainer program showed effects on attentional processes, memory, and emotional processing in people with early stages of schizophrenia, although it did not show transfer to daily life functioning and social cognition [40]. Finally, the study by Matsuoka et al. [41] evaluated the neurological changes after training with the cognitive remediation software Jcores VCAT-J; the authors found that this intervention induced microstructural changes in the posterior lobe of the left cerebellum, which were associated with changes in the verbal fluency of the participants.
Multiple sclerosis
In adults with multiple sclerosis, the most widely implemented training program was the Rehacom cognitive rehabilitation software, which was included in 6 studies [42-47]. Studies found improvements in measures of processing speed [42,43,46,48-50], verbal and visuospatial working memory [42-44,46,47,51-53], verbal fluency [44,46,47], visuospatial skills [46], attention [46,47,50,53], and general cognitive performance measured with the SDMT digit and symbol test. However, changes in many of these cognitive processes were not sustained after rehabilitation [45,43], while improvements in attention [42] and processing speed [46] were maintained after months.
The Cogni-track cognitive remediation program, based on computerized working memory exercises, and showing high adherence to treatment, improved working memory in patients with multiple sclerosis. The authors found that the intervention is more effective in programs supported by machine learning algorithms that allow activities to have an adaptive and progressive difficulty [51]. Also, studies in this population were conducted with Neuroracer [48], demonstrating effects on processing speed and psychomotor function. A novel Speed Processing Training (SOPT) program demonstrated a transfer effect close to the processing speed measured with WAIS-III [49]. With the Cogmed program [52], near-transfer effects were observed on working memory and far on several measures of attention, with a secondary effect on mood.
The work of Pérez-Martín et al. [50] evaluated a computerized novel training based on n-back combined with self-training at home to reinforce cognitive strategies; the intervention showed positive effects on attention, working memory, and processing speed, with transfer effects on mood. One study compared the effectiveness of computer-based (Captain's Log, Mindpower), manual, and combined cognitive rehabilitation, but the authors did not find that all three approaches showed effectiveness in rehabilitating working memory, executive function, processing speed, and selective attention in subjects with multiple sclerosis. However, they did not find superiority of one approach over the other, concluding that all three are equally effective [53].
Depression and anxiety
In another population studied, young adults and middle adults were patients with depressive disorders. Most studies found positive effects of different programs on executive functioning in general [54-56] and some specific executive functions. In patients with major depressive disorder, a clinical trial with the Cogniplus program significantly improved attentional processes and strengthened adaptive and socialization skills [57]. In this same population, the computerized game-based program PEAK led to improvements in executive functioning and processing speed with no effect on depressive symptoms [54], and intervention with the Cogmed working memory training platform improved executive function, processing speed, and emotional working memory [55].
Their clinical trial [56] compared goal management training with computerized training. The study showed that the former was superior to the latter in reducing everyday executive dysfunction, with effects on symptom reduction at a six-month follow-up.
In anxiety disorder individual's adaptive n-back training led to improvements in WM, with transfer to the reduction of self-reported worry and anxiety symptoms [58]. In people with emotional disorders related to stress, advanced gaze contingent attention training led to significant improvements in selective attention, while generating several beneficial effects: increased attention to positive over negative information, greater reappraisal ability to regulate negative emotions, and reduced state rumination compared with the control group [59].
In adults with post-traumatic stress, cognitive-affective training with a gamified PEC-SCA did not show a generalized benefit on EF or symptoms [60]. Lumosity showed improved performance for participants who received working memory training and yoga than those who received working memory training alone. The improvement of group 1 participants in working memory skills is possibly due to the additional benefits of yoga [61]. Lumocity was also studied in veteran combatants with post-traumatic stress disorders; home-based cognitive training demonstrated feasibility, adherence, and satisfaction in participants. Such training also led to improvements in self-perceived executive functions, as well as subjective improvement in symptoms of depression post-traumatic stress [62].
Acquired brain damage
In adults with acquired brain injury, we found two clinical trials evaluating the BrainGymmer program: one of the studies showed an improvement in cognitive flexibility after the intervention [63], while a second study carried out by the same authors, although improvements were recognized in some EFs, they occurred both in the intervention group and in the control groups, suggesting that the improvement was due to non-specific training effects [64]. Nor was there any evidence of effects on any cognitive function associated with the intervention with Cognifit in the same population [65].
Another study with the Erica cognitive remediation platform showed improvement in attention and memory capacity in the intervention group, with benefits in mood in patients with ischemic or hemorrhagic stroke [66]. An RCT compared a paper-and-pencil intervention with Rehacom, finding superiority in the latter's effects in favoring sustained attention and working memory [67]. In patients with subacute stroke, a clinical trial found that training of 6 to 10 sessions with virtual reality activities based on tasks of daily living led to improvements in flexibility, inhibition, conceptualization, programming and memory, and global cognition [68].
In patients with stroke, a virtual reality environment for prospective memory rehabilitation showed a significant improvement in prospective memory skills, which remained stable four weeks after treatment [69]. Power AFA software is successful in improving language and cognitive recovery in patients with post-stroke aphasia in the chronic phase [70]. In a study of patients with traumatic brain injury, impaired attention, and executive control, improvements in attention regulation were observed following an intervention with APT - Attention Process Training-Based Cognitive Training [71].
Substance abuse-associated disorders
Different programs based on computer systems have also been investigated in disorders related to the abuse of psychoactive substances. In an intervention with Cogmed, improvements in verbal working memory function were found in patients with histories of drug abuse, but did not show transfer effects to other cognitive processes, nor did it reduce symptoms of drug abuse [72,73].
The effects of the computerized program Curb Your Addiction were studied in patients in the process of rehabilitation for methamphetamine use, finding improvements in working memory in addition to traditional treatment. Additionally, it was shown to reduce clinical symptoms of impulsivity and improve self-regulation [74]. This same program in patients with substance abuse disorder was associated with increased volume in mesolimbic reward regions that coincided with improvements in impulsivity scores [75]. In this same population, an intervention with Lumosity was shown to improve performance in inhibition tasks, with an effect on quality-of-life indicators [76]. And a novel program based on Goal Management Training together with pharmacological treatment showed a significant effect on inhibitory control, with transfer to working memory and planning, as well as a reduction in impulsivity [77].
In recently detoxified alcohol use disorder patients, two versions of a novel n-back task-based program showed improvements in inhibition, with greater effects in the emotional version of training compared to training with neutral stimuli [78]. In adult smokers, a non-commercial computer program showed no significant effect on EF after it was applied [79].
Attention deficit hyperactivity disorder
Three studies on young adults with ADHD were identified. One of them [80] evaluated the effects of a computerized program of progressive attention training (CPAT) and found that the intervention group showed significant improvements in selective-spatial attention, as well as near transfer to executive attention, with effects that were sustained after follow-up, although with no effect on self-reported ADHD symptoms. The other two studies evaluated the Cogmed working memory training platform. In one of them, the training effects were small [81], while the other study showed improvements in working memory tasks, without transfer effect nor differential effects in longer interventions compared to short interventions. However, the participants of the extended version of the intervention demonstrated greater use of strategies and not only of solving tasks [82].
Other clinical conditions
In adults with cognitive impairment, HappyneuronPro generated improvements in executive functioning, increased frontal theta power, and reduced posterior alpha EEG power at two weeks of training [83].
In patients with obsessive-compulsive disorder, an intervention with Cogtrain, a program designed by the National Alliance for Research on Schizophrenia and Depression, generated improvements in Executive Functioning and processing speed and contributed to the reduction of cognitive depressive symptoms [84].
Regarding surviving cancer patients, two studies report an evaluation of the feasibility and effects of cognitive training with Brain HQ: Wu et al. [85] found that although the program was shown to be feasible and highly acceptable, it only showed benefits on reaction time, while Von et al. [86] found that both computerized cognitive training programs and remotely administered active attention control computer programs are feasible, as they generate small positive effect size and adherence on cognitive processes exercises.
The pilot study by [87] evaluated a program based on video games called Mycognitivon in cancer survivors with cognitive impairment; the intervention group showed that memory, perception, and motor function had a different evolution in the intervention group, showing less deterioration compared to the control group. An intervention with the HappyneuronPro program in women with breast cancer generated improvements in memory and concentration, verbal learning, and WM, which were maintained after five months [88].
Two studies were found in patients with Huntington's disease. In one of them, a multidisciplinary rehabilitation intervention integrated with aerobic exercises, computerized cognitive training (Neuronation) and dual-task training and sleep hygiene, and nutritional guidance, led to significant improvements in verbal learning and memory, attention, flexibility, cognitive, and processing speed in the intervention group compared to the control group [89]. At the same time, the second study developed with the HappyneuronPro program, while showing adherence in one group of the sample, did not achieve widespread feasibility in the sample as a whole [90].
In two clinical trials [91,92], the effect of computer-based cognitive remediation programs was evaluated in patients with HIV, one of them implemented an intervention with Lumosity [92], and in another, an intervention with PSSCogRehab [20]. Both interventions studied led to reducing the working memory deficit in these patients.
Healthy population
As mentioned above, 4 of the studies were conducted in a healthy population of average adults, while in young adults, 20 were identified, most of them in university students.
Programs based on the n-back paradigm were one of the most frequent to train working memory [93-97] and showed transfer effects to other processes such as attentional control [95], cognitive flexibility [97], inhibition [95,97], dual tasking [94], reaction time [98], and visual short-term memory [95] in healthy adults. In studies with healthy adults, training based on other classical tasks such as the Stroop test [99,100], the Flanker test [100], and other classical tasks [100-102] has also been recognized. Commercial computer training programs such as Lumosity [103-104], Cogmed [105], Mind frontiers [106-108], and Gwakkamole app [109] have been identified as well. Also, novel programs designed by researchers [110-114] have been remarked.
One of the commercial programs based on the n-back paradigm was Brain Twister2, an ascending complexity scheme that generated increasingly complex training demands. Interventions based on this program demonstrated greater near transfer to untrained working memory tasks and far transfer to attentional control [115]. Some authors found that in task-based n-back training, the improvements seemed restricted to tasks like those trained in working memory, but without transfer to other cognitive processes [93,94,116]. While other programs, based on strategies and not on tasks, showed greater transfer to other untrained tasks [96,100].
Three studies used training with the Mind Frontiers serious game-based cognitive stimulation program. Zwilling et al. [106] observed effects of near transfer to working memory tasks and far transfer to perceptual speed tasks in an intervention with this program in healthy young adults, while Baniqued et al. [107] found similar near transfer to working memory tasks and far from processing speed and reaction time. In another study, Mind frontiers showed transfer to decision-making and general executive functioning, with greater effect when combined with other programs such as meditation and high-intensity cardio resistance training [108].
On the other hand, in an intervention with Lumosity, improvements were observed in cognitive flexibility, attention, and reaction times, although these changes were not reflected in evoked potentials [104]. An fMRI study demonstrated that a novel executive control training intervention based on the Flanker task caused an increase in amygdala-IFG connectivity, further showing improvements in inhibitory control, attention, and emotional regulation [100]. A study contrasted a novel program based on classical tasks to train working memory by comparing a linear scheme and one with progressive difficulty. The authors concluded that cognitive training programs should incorporate adaptive task difficulty to enhance the transfer of training gains and maximize the efficiency of task-related brain activity [117].
Some studies that implemented working memory training, such as Cogmed [105] and other non-commercial programs created by the researchers [114,118], showed improvements that were restricted to specific working memory tasks without no other near and far transfer effects. In this vein, training with MultiTask also did not show significant effects on working memory, cognitive flexibility, or inhibition [119]. Another working memory training program such as Neuronation showed effects on trained working memory tasks, but also showed substantial improvements in near transfer tasks to other domains of working memory [120]. Some inhibition training programs, such as Gwakkamole [109] and other novel programs [112,113], did not significantly affect inhibition or transfer to other domains, such as working memory, cognitive flexibility, and planning. While Namratha et al. [101] found that working memory training in healthy average adults achieves greater results when combined with yoga training. Task repetition-based training demonstrated close transfer to similar tasks but no transfer effect to inhibitory control [118].
Discussion
This scoping review aimed to provide an overview of the evidence collected to date on computer-based cognitive stimulation and rehabilitation programs for executive functions applied in young and mid-adulthood. The main finding of this scoping review was that most studies on the use of computer-based cognitive training programs had shown favorable results on executive functions in young and middle adults.
The executive functions of working memory, attention, processing speed, and inhibitory control were the most studied in the population between 18 and 60 years of age. Working memory has been the most studied executive function also in other population groups [93,111]. In this scoping review, in addition to being the most frequent, it is also the executive function that showed the greatest benefits of cognitive training programs mediated by computer systems and in which greater effects of near and far transference were recognized both in healthy and healthy populations, which demonstrated that training in this cognitive domain could benefit the development of other cognitive abilities, such as reasoning skills, mental focus in daily activities, multitasking, and attention.
Rehabilitation and stimulation of other executive functions, such as cognitive flexibility, planning, verbal fluency, inhibitory control, and emotional regulation, were less frequent, and the effects on inhibitory control generally showed more limited effects [33,109]. These results show an important knowledge gap in future research and intervention designs mediated by computer systems.
A large part of the studies in healthy young adults was carried out on university students [98,105,110,112,114-116]. In these, the participants generally belonged to the same university that led the study, situation which can lead to a significant bias since when doing a convenience sampling with a captive population, although the risk of dropout in the study is minimized, it limits the results to the sociodemographic characteristics of that population.
Among the populations with the most studied clinical conditions in young and middle adults were multiple sclerosis [42-50,53], schizophrenia [30-39,41,67], acquired brain injury [63-65,67,69,70], substance use disorders [72-78], and depressive disorders, [32,54-57,78] and a minority of studies were conducted in young adults with Huntington's disease [89,90], stress-related emotional disorders [59-62], and cancer survivors [80,86-88]. Many of these studies evaluated the effects of interventions on the executive functions of sustained attention, concentration, and speed of information processing.
Regarding the effects of the interventions, the review shows varied results and, in some aspects, contradictory. Although most of the studies showed effects of near transference that, for the most part, ranged from moderate to significant, other programs studied did not show the expected effects or showed a very limited transference, especially in the effects of far transference, which indicates that the degree of generalization is limited in these intervention programs [20], as reported by Etherton et al. [105], who in their results found that working memory training with the Cogmed program does not improve performance on unrelated tasks or improve other cognitive abilities. From these results, some researchers conclude that the effect of distant transfer after executive function training is far from clear.
Research has found multiple benefits of integrating computer systems into cognitive stimulation and rehabilitation in adults. The use of online access platforms allows the professional in charge of the intervention to have a wide range of activities to select, manage, and schedule, which permits them to design personalized work sessions and record the evolution of the subject. Some of these platforms have digital test batteries and machine learning modalities that provide "intelligent tutoring" [104], giving instructions, accompaniment, and constant feedback to the subject and the personnel in charge of care. The clinical interventions showed better effects when accompanied by sessions at home; access to the computerized program from multiple devices precisely provides continuity to the clinic from home or another location without requiring special equipment. This characteristic had a favorable impact on retention and adherence to treatment while allowing the optimization of technological and human resources, since it allows individual but simultaneous intervention with several subjects simultaneously.
The computerized machine learning algorithms take the data of the person's performance and learn from this data to adapt to the complexity of the activities and provide a training scheme with ascending and progressive complexity, this being one of the most outstanding and best characteristics results in interventions [51]. Clinical interventions showed better effects when they included game-based, adaptive, challenging activities of increasing complexity and in highly motivating environments [51,58,83,119]. The researchers suggest that future interventions look for ecological validity in the design of the activities, so that the tasks represent the problems that adults face in their daily lives [71,120]. Several studies agreed that the greatest benefits were obtained by people with lower levels of cognitive impairment at the time of the pretest, which may be due to a ceiling effect [32].
Some research found that the improvement in some domains was not due to a specific improvement in that domain, but rather a consequence of the more efficient and strategic use of the cognitive skills learned during training. They also identified that considerably better results are obtained by combining the intervention based on tools and computational skills with training in metacognitive strategies and problem-solving [50,61,100]. Therefore, this may be a promising research field for further study.
Conclusions
Following the above, in most studies, interventions mediated by computer systems are effective in stimulating some executive functions in young and middle adults. However, these findings also demonstrate the need to study computer-based treatments for other clinical and subclinical conditions in young and middle adults with impaired executive functioning that have not been addressed in empirical studies and include follow-up measures in the methodological design of the studies. It is necessary to carry out more studies in young and middle adults with other diagnoses, such as mild cognitive impairment, obsessive-compulsive disorders, anxiety disorder, neurodevelopmental disorders, and intellectual disability, among others, since few studies were identified in the reviewed literature.
Finally, based on the results of this review, it was possible to collect an important corpus of studies on the effects of rehabilitation and stimulation of executive functions in young and middle adults with programs mediated by computer systems. However, the absence of Latin American publications in this population was evident. Therefore, the authors suggest, for future research, the development of a systematic review and meta-analysis that allows the evaluation of the size of the effect, the quality of the studies, and biases. For future studies, the authors suggest that the tasks be designed to train multiple cognitive skills and not specifically focus on task performance.

