











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Voice disorders are a significant work-related health issue among teachers [1,2], with detrimental socioeconomic consequences and negative effects on student performance [3-5]. Moreover, as teachers serve as communicative models for their pupils, voice disorders can also affect the voice production of students who may try to imitate their teachers [6]. Unhealthy voice models may lead to voice disorders among children, negatively impacting their health and quality of life.
Multiple factors can contribute to the development of voice disorders. Previous research has indicated that individual factors such as age, gender, and work-related factors such as the number of students per classroom, years of experience, and topic of teaching, as well as environmental factors such as noise, reverberation time, temperature, and humidity, can all play a role [1,7-10]. Classroom acoustics, including noise and reverberation time, have been shown to be strongly associated with the increased occurrence of voice disorders among teachers [11,12].
Furthermore, previous studies have reported various interventions to treat voice disorders among teachers, including voice amplification, individual voice therapy such as vocal function exercises, resonance therapy, and respiratory muscle training [13-15], as well as vocal hygiene instruction [13,16]. However, these interventions often neglect to consider the environment as a potential risk factor for voice disorders, or the children as active participants in teaching activities and communication processes within the classroom.
Moreover, to effectively address the issue of voice disorders among teachers, it is important to consider the hierarchy of hazard control for background noise and reverberation, which are two conditions strongly related to voice disorders. This hierarchy involves a series of steps, starting with the elimination of the hazard, followed by substitution, engineering controls, administrative controls, and personal protective equipment provision [17-19]. In the case of background noise inside the classrooms, elimination would involve removing the noise source inside the classrooms and schools, while substitution would require replacing the noise source to reduce noise levels. However, both steps may not be feasible given the influence of pupils on noise levels inside the classrooms and schools. Engineering controls, such as isolating teachers from noise conditions, providing rest areas, and designing options that reduce noise, may be expensive for schools to implement. The next step is administrative controls, which include warning teachers about restricting access to noisy environments, providing training, and adjusting the working process. Finally, personal protective equipment provision may involve delivering earplugs to control exposure to noisy conditions or providing amplification systems to avoid the need for teachers to scream during teaching.
Unfortunately, interventions for voice disorders among teachers commonly focus solely on the worker (teacher), without considering the influence of the work environment on the onset of voice disorders. This narrow focus may be one of the reasons why we still have a high occurrence of voice disorders among teachers. Therefore, it is crucial to follow the hierarchy of hazard control and consider the work environment when designing interventions to ensure a safe workplace for occupational voice use.
Implementing interventions following the hierarchy of hazard control can be challenging, especially when the elimination or substitution of the hazard is not feasible. An alternative approach to addressing voice disorders among teachers is through Workplace Health Promotion programs (WHPPs). The WHPPs aim to prevent, minimize, and eliminate health hazards while promoting work ability, which means maintaining a physical, mental, and social balance of workers' health [20]. The workplace is considered a good setting for public health promotion because workers spend long periods at work and build natural social networks [21]. The roots of health promotion can be traced back to the 17th century when an Italian physician, Bernardino Ramazzini, commented on the poor health of cobblers and tailors who worked in poorly lit conditions [22]. In the years after World War II, worksite health promotion programs began to take shape, stemming from executive fitness programs started by business managers who recognized the benefits of a healthy lifestyle. These programs were initially restricted to upper management but were later offered to employees of all job levels in the 1970s, leading to a shift towards broad health issues. This shift was accompanied by organizational changes within companies, such as strengthened relationships between occupational medicine and human resources, and the establishment of the Association for Worksite Health Promotion [23].
From the Workplace Health Promotion approach, workers are encouraged to play key roles in promoting health and well-being [24,25]. Therefore, WHPPs can be a valuable tool for reducing voice disorders among teachers. These programs can involve a variety of interventions, such as workplace environmental modifications, training, and education programs, and health behavior change initiatives. For example, WHPPs can include the implementation of strategies to reduce background noise and reverberation, such as acoustic panels and other engineering controls. Additionally, WHPPs can provide education and training to teachers on vocal hygiene and voice care practices, as well as stress reduction techniques that can reduce the risk of voice disorders. By involving teachers in the design and implementation of these interventions, WHPPs can help to create a culture of health and well-being in the workplace, leading to improved voice health and overall worker health.
With this in mind, the objective of this study was to determine the effect of the implementation of a workplace vocal health promotion program (WVHPP) in a Colombian primary school. The WVHPP included the use of a noise traffic light inside the classroom, in addition to training sessions for pupils and their teacher on the effect of noisy conditions on voice production, and healthy ways to use their voices during and outside classes.
Method
Design and participants
This pilot longitudinal study was conducted over one month in 2019 to assess the effectiveness of a Workplace Vocal Health Promotion (WVHPP) program among elementary school students and their teacher. Institutional Ethics Committee approval was obtained before participant recruitment. Written informed consent was obtained from the teacher and parents, while children and their parents provided assent. Convenience sampling was used to recruit participants from a public school in Bogotá, Colombia, with high background noise levels due to its proximity to main streets and an open gym located in the middle of the building. The latter caused noise from sports classes to be heard by teachers and students in surrounding classrooms. Pupils from the second grade of elementary school and their teacher participated in this study. Participants underwent three repeated measures: (1) before implementation of the WVHPP (first week of follow-up), (2) during the implementation of the WVHPP (third week of follow-up), and (3) at the end of the WVHPP implementation (fourth week of follow-up). However, some children did not complete the second follow-up measurement due to absence from school on the day of the assessment. A voice sample of connected speech was recorded from all participants during each of the three-time points.
Data collection procedures
Voice samples and equipment
Voice recordings were obtained from participants using standardized procedures. The teacher read the first six sentences of El caballero de la armadura oxidada (The Knight in Rusty Armor) [26] in a conversational pitch and loudness, while children were asked to describe an illustration of a language protocol (PLON-3 AGE) [27].
Recordings were made in a low background noise room in the school, with ambient noise levels measured at approximately 29 dB(A). An omnidirectional microphone (AUDIOART-DYNAMIC VOCAL MICROPHONE ART-139) was positioned 10 cm from the participant's mouth to capture the speech signal. Recordings were captured using an Olympus VN-960PC Digital Voice Recorder and subsequently transferred to a PC for analysis using Praat software.
Voice parameters
In this study, we analyzed voice samples collected from the participants using five voice parameters: fundamental frequency, the standard deviation of the fundamental frequency, vocal sound pressure levels, the standard deviation of sound pressure level, and cepstral peak prominence smoothed. Fundamental frequency (fo) represents the number of times the vocal folds open and close per second and is expressed in Hz. The range of frequencies produced by the human larynx varies depending on age and sex [28]. We used the “mean pitch” reported in the “voice reports” section of Praat as the value of fundamental frequency during each production. The standard deviation of fundamental frequency (fo SD) measures the dispersion of a set of data values and, for fo, it shows its amount of variation during speech production [29].
Sound Pressure Level (SPL) is defined as the amplitude of the wave of sound produced when a voice is transmitted in the air medium [28]. We used the “Get intensity” function to obtain the value of the mean energy intensity (sound pressure levels) during each production. The standard deviation of vocal sound pressure levels represents the dispersion of the amplitude of the wave of sound produced when voice is transmitted in the air medium.
Cepstral Peak Prominence Smoothed (CPPS) is a measure of the degree of harmony during phonation. The more periodic the signal, the greater the harmony, and, therefore, the CPPS. One strength of CPPS is that it does not rely on pitch tracking and tends to produce valid and reproducible values even for very aperiodic voice signals [30,31].
These parameters were chosen based on previous studies that reported a significant association between vocal fatigue and fundamental frequency [32,33], the standard deviation of the fundamental frequency, vocal sound pressure levels, and the standard error of vocal sound pressure levels [32,34]. Cepstral peak prominence smoothed was also included as a good indicator of voice quality [35,36].
Workplace Vocal Health Promotion Program (WVHPP)
The WVHPP was designed with two primary goals in mind: to reduce noisy conditions inside the classrooms that may cause loud voice production, which has been found associated with voice disorders among teachers and students, and to increase awareness about the effect of background noise on voice production. To achieve these goals, this program was delivered face-to-face in the actual classrooms where classes occurred, and all sessions were conducted in the afternoon. To accommodate school policies and the schedules of teachers and students, the WVHPP had a total duration of four weeks, including a follow-up measurement. Despite the program's relatively short duration, we ensured that all essential components and activities were included to guarantee its effectiveness in enhancing the voice health of participants.
During the first week of the study, two preliminary meetings were held with the participants. In the first meeting, the researchers presented the study to the pupils and their teacher, answered their questions, sent to the children's parents the assent and consent forms, those participants that accepted to participate, signed and sent back the forms. During the second meeting, the teacher and children completed a self-reported questionnaire (data not shown), which included questions on the voice-related quality of life, voice functioning, and voice symptoms. The teacher's questionnaire was based on previous research [37], while the pupils' questionnaire included the Spanish translation of the pediatric voice-related quality of life [38]. Also, the teacher and her students recorded a voice sample of connected speech to calculate a baseline measure of voice parameters. In this first part, we included both teacher and students who consented and assented to participate. In addition, a checklist was used to identify associated factors of voice problems presented during lectures. This checklist was filled in by the researchers through direct passive observation (data not shown).
During the second week, we conducted two sessions of the WVHPP with the assistance of two speech-language pathologists as research assistants. Each session lasted approximately one hour. The first session comprised five parts. In the first part, participants, including pupils and their teacher, received information about how voice is produced. This information was presented to the participants using images of the larynx, which were presented to the participants, allowing them to identify the key structures involved in voice production. In the second part, participants were requested to locate their larynx and to feel the changes that occur when they breathe, talk, swallow, or scream. They then shared their perceptions with the group. The third part of the session involved highlighting various sources of noise in the classroom, including external sources, chairs, tables, and even screaming. Participants were then requested to identify which of these elements were present during their classes. In the fourth part, researchers discussed the impact of noisy environments on voice production, including the Lombard effect, and demonstrated how people tend to increase their volume when communicating in noisy environments. In the last part of the session, researchers emphasized the importance of voice care and hygiene, such as avoiding screaming, drinking water during classes, speaking at closer distances rather than screaming from one end of the classroom, and reducing background noise in the classroom.
During the second session of the WVHPP, participants were trained on how to monitor noise levels inside the classroom using a mobile app called "Sound Meter Decibel" by Sprint Coder (2014). The teacher was requested to download the app on her mobile phone, and the researchers calibrated the app with a professional sound level meter called Smart Sensor As824 before using it. The app displayed a "noise traffic light" that changed colors based on the noise levels in the classroom, with green indicating low levels, yellow indicating moderate levels, and red indicating high levels. To familiarize the participants with the app, the teacher placed her phone on the frontal wall of the classroom, and the students were asked to produce different noise levels (e.g., very quiet, chatting, loud talk, screaming) and observe how the "noise traffic light" changed color.
Additionally, the researchers designed a "paper noise traffic light" that was used as a monitoring tool for daily noise conditions. The students and the teacher were instructed to put a star on the green smiling face in the "paper noise traffic light" if the classroom was under low noise conditions during lectures, one star on the yellow worried face if the class had some moments of noise but also some silent moments, or one star on the red crying face if the class was very noisy during the day. As an administrative measure, the researchers appointed a "captain" per group of students. The "captain" encouraged their classmates to keep noise levels low during classes when the "noise traffic light" was yellow or red.
During the third week of the study, we conducted the first follow-up measure, which occurred one week after the implementation of the WVHPP. Similarly, during the fourth week, we conducted the last follow-up measure after the completion of the WVHPP. To ensure that the information about the WVHPP is presented clearly and comprehensively, we followed the Template for Intervention Description and Replication (TIDieR) checklist [39]. Table 1 presents detailed information about the WVHPP, which can serve as a valuable resource for researchers and practitioners interested in implementing similar interventions in their settings.
Table 1 Template for Intervention Description and Replication (TIDieR) checklist of the PTS Program.
| TIDier item | Description |
|---|---|
| Brief name | Workplace Vocal Health Promotion Program |
| Why | The hierarchy of hazard control establishes that interventions should start with the (1) elimination of the hazard, followed by (2) substitution, (3) engineering controls, (4) administrative controls, and, as a last step, (5) personal protective equipment provided. The WVHPP implemented elimination and administrative controls to lower noisy conditions inside the classrooms, and therefore reduce the associated vocal demand and vocal demand response. As elimination control, we aimed to “remove” the noise source inside the classrooms and schools using reducing background noise levels. The use of the sound level meter mobile app allows to control of background noise levels, and as administrative control, the training developed during the program and the “student captains” allowed to identify high background noise levels and implement actions to reduce them. Moreover, we based our program on the Workplace Health Promotion approach that encourages teachers (and students) to play key roles in promoting health and well-being, considering the workplace an ideal scenario for delivering initiatives to promote health |
| What | |
| During the third week, we performed the first follow-up measure for the teacher, and during the fourth week, the last follow-up measure was performed | |
| Who provided | The sessions were implemented by two speech-language pathologists (research assistants) who had one year of experience. Both research assistants received four sessions of training by the principal investigator (first author) about the content, implementation, and organization of the program |
| How | This program was delivered face-to-face to the group of second graders and their teacher |
| Where | The program was implemented in the school. The pre-and post-recordings were performed in a silent room on the third floor of the school, whereas the WVHPP was implemented inside the classroom |
| When and How Much | The WVHPP was implemented for four weeks (one month). All the sessions were implemented in the afternoon. The program contained four sessions (two for voice recordings), and two implementation sessions. Each implementation session was about one hour in duration |
| Tailoring | The program was designed to be personalized to the group's knowledge and participation. Therefore, the research assistants prepared different contents about the topics to be covered during each one of the sessions, following participants' comments and questions the content were used |
| Modifications | The program was delivered as planned |
| How well | The program adherence was not assessed |
Data processing
To process the data, we used Praat software (version 6.1.30) [40]. The speech samples were recorded with a sampling frequency (fs) of 44,100 Hz. We applied a passband Hann filter with a bandwidth of 5 Hz to 10 kHz to the acquired signals to allow the passage of the main frequency components. The fundamental frequency (fo) was estimated through the pitch autocorrelation algorithm. We set the pitch floor and ceiling at 50 Hz and 500 Hz for the children's speech samples, and 70 Hz and 450 Hz for the female teacher's speech samples. From fo, we calculated the standard deviation of the fundamental frequency (fo SD) for all records. Additionally, we computed the standard deviation of sound pressure level (SPL SD).
Statistical analysis
Considering the objective of this study and the number of participants, our analysis plan aimed to identify changes in five dependent variables -fundamental frequency (fo), fo standard deviation (SD), Vocal Sound Pressure Levels (SPL), SPL SD, and CPPS- due to the WVHPP. The statistical analysis was performed in three steps. First, descriptive analysis was performed on the data recorded by the pupils and their teacher. Second, the normality of the data was assessed using the Kolmogorov-Smirnov test. Third, Generalized Estimating Equations (GEEs) were used to determine whether the WVHPP was associated with differences in the five dependent variables. The Generalized Estimating Equation (GEE) is a method used to estimate parameters in a statistical model with repeated measurements of the same subject. This approach is used when assumptions about the distribution of the response variable(s) are not completely known. The GEE method is particularly advantageous when the correlation matrix is misspecified, since it provides a consistent estimate for the regression parameter. The correlation matrix is used to describe the relationship between the repeated measurements, and when it is not correctly specified, it can lead to biased estimates of the regression parameter. The GEE method can correct this problem and still provide reliable estimates of the regression parameter [41]. All the models were controlled by the type of participants (teacher vs. students), and gender (male vs. female). The magnitude of the association was expressed by the beta (β) and its standard error (SE). All statistical analyses were performed employing SPSS 25 (IBM Corporation).
Results
Descriptive analysis of participants and voice parameters
In total, twenty-five pupils from the second grade of elementary school and their teacher participated. The age of students ranged between 7 and 9 years old; the gender distribution was nineteen boys (76%) and six girls (24%). The teacher was a female of 29 years old.
As shown in Figure 1, fundamental frequency (fo) decreased consistently during the WVHPP. Although, among the female participants (including the teacher), there was a slight increase at the end of the follow-up. Regarding the fo standard deviation (fo SD), female participants tended to decrease their fo SD during the program, whereas male participants decreased this parameter in the first follow-up, but it increased in the post-intervention measurement (Figure 2).
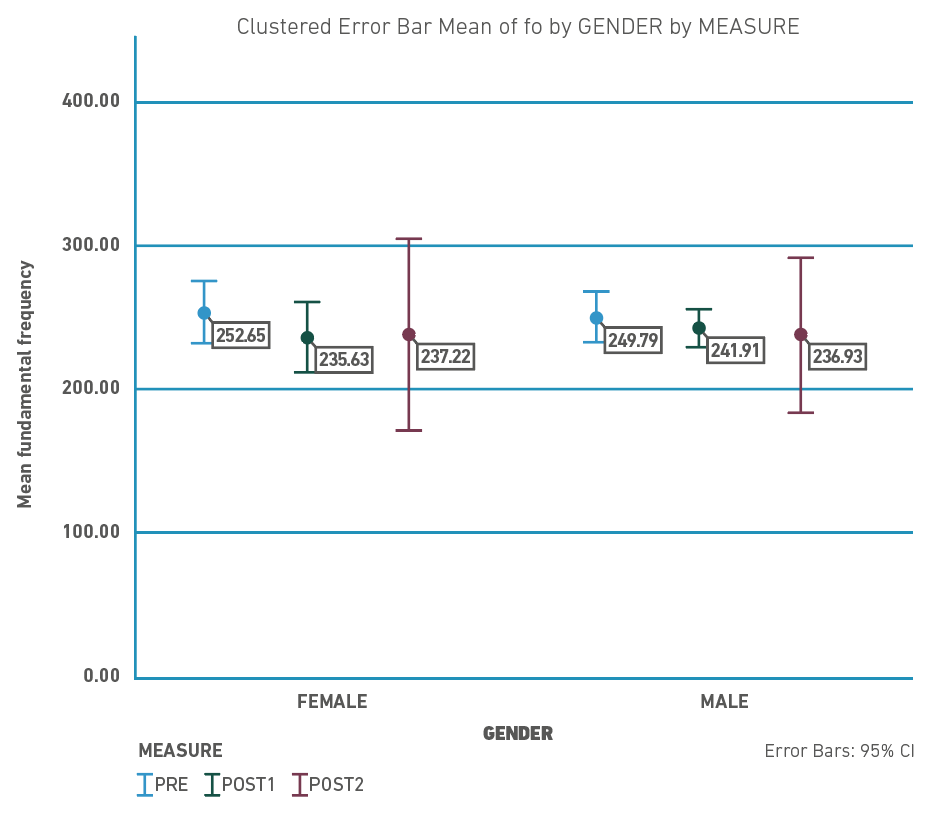
Figure 1 Changes in fundamental frequency mean per gender during the Workplace Vocal Health Program.
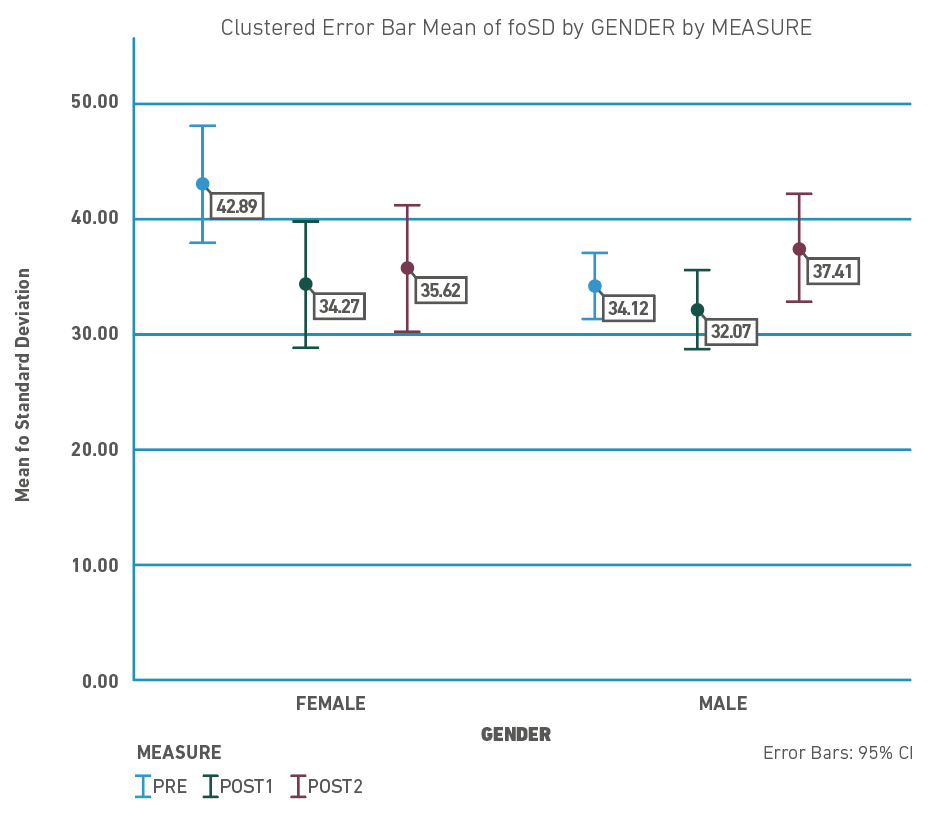
Figure 2 Changes in fundamental frequency standard deviation mean per gender during the Workplace Vocal Health Program.
Figure 3 shows the mean values of Sound Pressure Levels (SPL) per gender during the three assessments. Both groups tended to decrease their SPL, but this tendency was more consistent among males (around 2 dB in every measure) compared to females (5 dB in the first measure, 0.10dB in the second measure). Concerning the SPL SD, Figure 4 shows that both groups had a decreased SPL SD in the first follow-up measure, but this tendency did not remain towards the end of the follow-up.
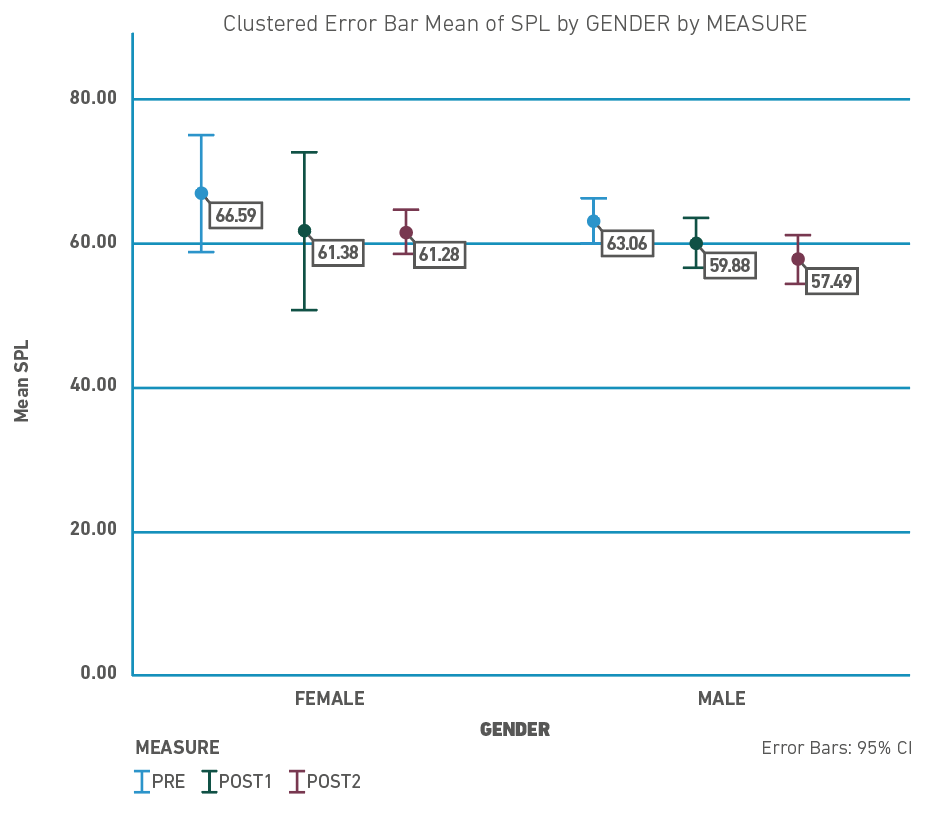
Figure 3 Changes in sound pressure levels mean per gender during the Workplace Vocal Health Program.
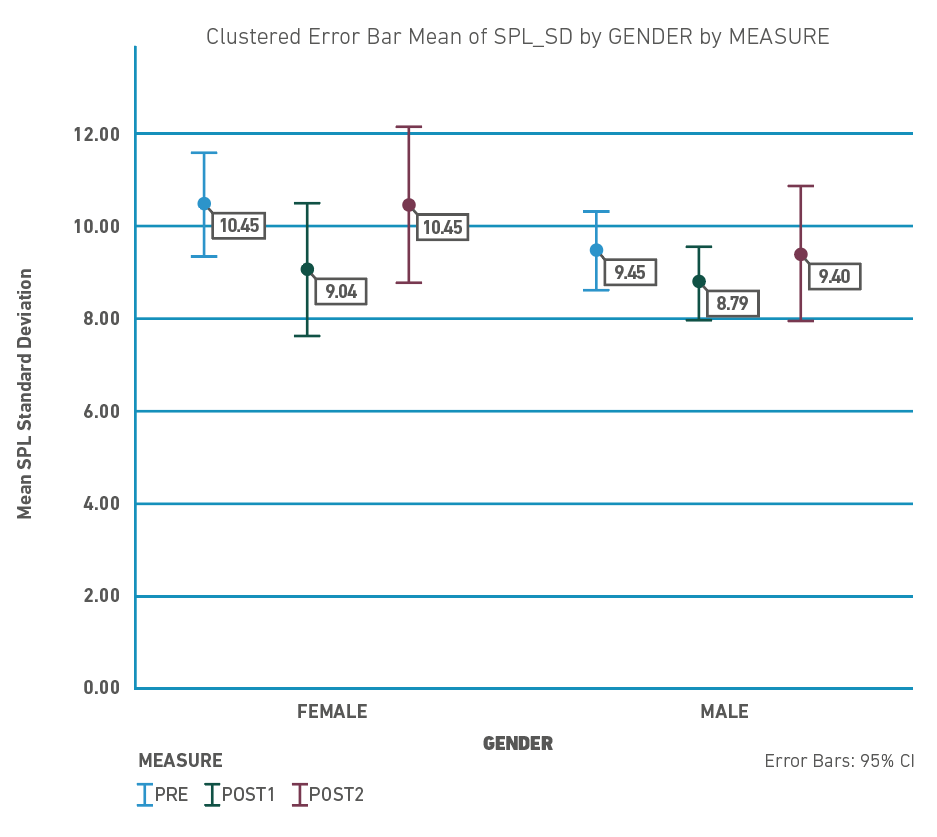
Figure 4 Changes in sound pressure levels standard deviation mean per gender during the Workplace Vocal Health Program.
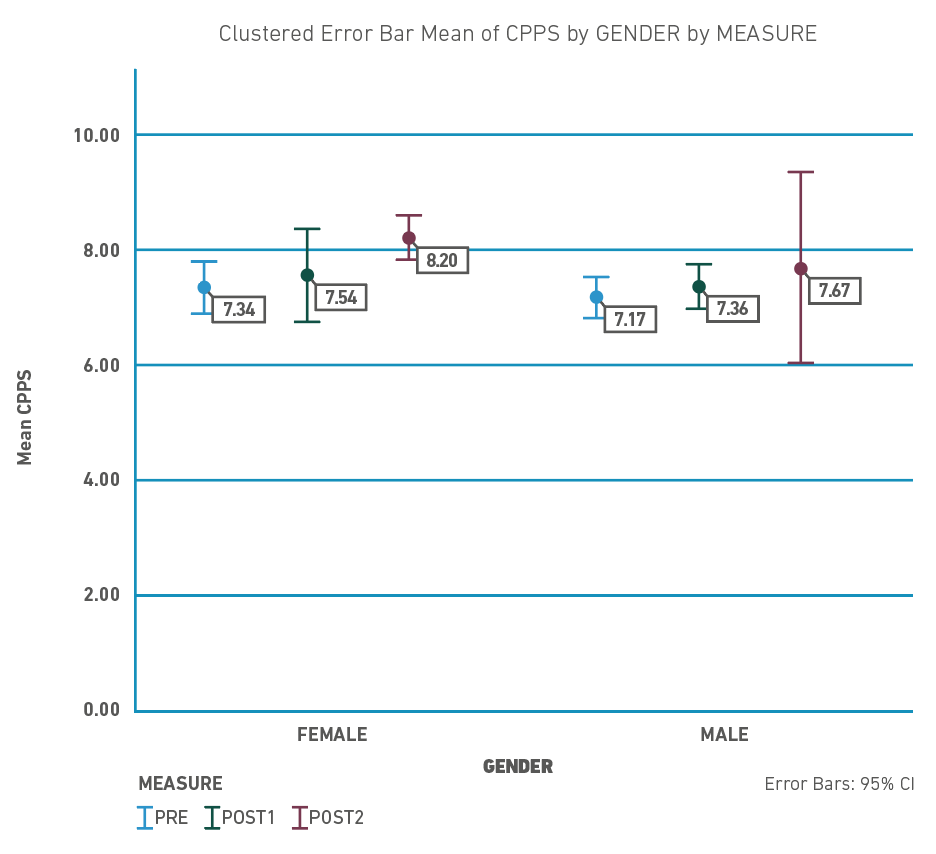
Regarding Cepstral Peak Prominence Smoothed (CPPS), as shown in Figure 5, there was a tendency in both groups towards increasing this parameter comparing the baseline measure with the post-intervention measure.
Effect of Implementation of a WVHPP on voice acoustic parameters
To determine the effect of the WVHPP on fundamental frequency (fo) and vocal sound pressure levels (SPL), we performed Generalized Estimating Equations. The models included three independent variables: gender (male and female), type of participant (teacher and students), and measure (baseline, first follow-up, and post-intervention follow-up).
As shown in Table 2, the WVHPP decreased fundamental frequency (fo) to 10Hz during the first week, and 6Hz at the end of the follow-up. This effect was statistically significant after controlling by gender and type of participant. Gender was not statistically associated with this parameter, whereas the teacher had a lower fo compared with her pupils (B= -90.04Hz). A similar tendency was observed when analyzing the Sound Pressure Levels (SPL), where the WVHPP decreased SPLs to 3.70dB during the first week, and 14.85dB at the end of the follow-up. This effect was statistically significant after controlling by gender and type of participant. Gender was not statistically associated with this parameter (p-value >0.05), whereas the teacher spoke louder compared with her pupils (B= 21.35dB).
Table 2 GEE analysis of the effect of the WVHPP on participants' voice parameters (all the models were controlled by gender and type of participant)
| Variables | Fundamental frequency | Fundamental frequency SD | Sound Pressure Levels | Sound Pressure Levels SD | Cepstral Peak Prominence Smoothed | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | p-value | B | SE | p-value | B | SE | p-value | B | SE | p-value | B | SE | p-value | |
| (Intercept) | 250.58 | 7.98 | 0.00 | 32.70 | 1.76 | 0.00 | 63.24 | 1.55 | 0.00 | 9.78 | 0.64 | 0.00 | 7.14 | 0.20 | 0.00 |
| Measure | |||||||||||||||
| Baseline Measure | Reference | Reference | Reference | Reference | Reference | ||||||||||
| First follow-up | -10.25 | 3.97 | 0.01 | -3.76 | 1.26 | 0.00 | -3.70 | 1.23 | 0.00 | -0.86 | 0.43 | 0.05 | 0.20 | 0.14 | 0.17 |
| Second follow-up | -6.48 | 2.76 | 0.02 | 0.64 | 1.52 | 0.67 | -14.85 | 1.17 | 0.00 | 0.97 | 0.64 | 0.13 | 0.17 | 0.22 | 0.43 |
| Gender | |||||||||||||||
| Male | Reference | Reference | Reference | Reference | Reference | ||||||||||
| Female | 12.68 | 9.58 | 0.19 | 14.18 | 4.13 | <.001 | -0.23 | 3.40 | 0.95 | -1.02 | 1.54 | 0.51 | 0.16 | 0.59 | 0.79 |
| Type of Participant | |||||||||||||||
| Students | Reference | Reference | Reference | Reference | Reference | ||||||||||
| Teacher | -90.04 | 8.36 | 0.00 | 0.41 | 4.60 | 0.93 | 21.35 | 2.80 | <.001 | 5.35 | 1.07 | <.001 | 0.92 | 0.53 | 0.08 |
Regarding the effect on fo standard deviation (SD), there was a decrease in this parameter in the first follow-up (B= -3.76), but the effect did not remain by the end of the follow-up. Gender was statistically associated with this parameter (B= 14.18), whereas the type of participant was not an associated factor (p-value >0.05).
Concerning the SPL SD, the WVHPP influenced this parameter during the first follow-up (B= -0.86; p-value= 0.05) but the effect did not remain at the end of the follow-up (B= 0.97; p-value= 0.13). Gender was not statistically associated with this parameter (p-value= 0.51), whereas the type of participant was an associated factor (B=5.35; p-value <0.01).
The WVHPP did not show any significant effect on the Cepstral Peak Prominence Smoothed (CPPS). After controlling for gender and type of participants, the model did not show any association between these variables and CPPS.
Discussion
This pilot longitudinal study aimed to determine the effect on voice parameters in pupils and their teacher of a three-week Workplace Vocal Health Promotion Program (WVHPP) in a school setting. With this in mind, we used the Generalized Estimating Equations to determine whether the WVHPP was associated with differences in five voice parameters (fo, fo SD, SPL, SPL SD, and CPPS). Two main results were found. First, the WVHPP had a statistically significant effect on fundamental frequency, the standard deviation of the fundamental frequency, sound pressure levels, and vocal sound pressure levels. Second, there was no statistically significant effect on the CPPS of the WVHPP.
Concerning the changes on fo, our findings on the decrease in fundamental frequency and fo SD after implementing the WVHPP are consistent with de Pina Pereira et al. (2015), who also observed a decrease in fundamental frequency following warm-up training [42]. However, our results contradict another study that reported an increase in fundamental frequency after a short voice training program for teachers [43]. Previous studies have suggested that increased fo after vocal demanding tasks may be an indication of vocal fatigue [32,44-46]. This suggests that vocal fatigue may result from increased muscle tonus as an adaptation to loading [47,48]. Based on the physiology of voice production, it can be inferred that lower values of fo post-implementation of the WVHPP may indicate a positive effect of this program on reducing vocal fatigue among pupils and to some extent, their teacher.
The decreased standard deviation of fundamental frequency observed post-implementation of the WVHPP may be indicative of improved laryngeal settings to avoid vocal fatigue. It is possible that the teacher and her students produced fewer variations in their pitch during speech as a means of better controlling their productions and reducing vocal effort and fatigue. However, further research is necessary to confirm these findings and to explore the underlying mechanisms behind these changes.
Our study found that implementation of the WVHPP resulted in a decrease in vocal sound pressure levels (SPL) and SPL SD among pupils and their teacher. Furthermore, there was an increase in the standard deviation of SPL among the teacher post-implementation of the WVHPP. The WVHPP included the use of a mobile App that functioned as a "noise traffic light" to control the loudness inside the classroom. Our results suggest that this tool, in combination with the use of a "paper noise traffic light," had a positive effect on reducing the loudness of both the children's and teacher's voices during conversation. The WVHPP also included active involvement of pupils, which was deemed as a strong component of the program by the participating teacher. While our study's results are promising, further research with background sound level measures during lectures and larger sample sizes are recommended to validate these findings.
Regarding SPL SD, previous studies have shown that teachers with higher standard deviations are less likely to report voice complaints [34] and vocal fatigue [32]. Interestingly, pupils had an opposite tendency to their teacher in terms of the standard deviation of the SPL, indicating a decreased spread of average SPL. This difference may be explained by the different types of voice used in the classroom. Teachers need to use a projected voice to ensure that they are heard by all students in the room, whereas pupils generally use a conversational voice to communicate with their peers and teachers. Therefore, the WVHPP may have had a positive impact on both teachers and pupils, reducing vocal effort and the risk of vocal fatigue. However, further research with larger sample sizes and measures of background noise levels during lectures is needed to confirm these results.
This pilot study has important implications for understanding the consequences of voice disorders in the classroom from an educational perspective. As oral communication is the primary means of knowledge exchange and construction in the classroom [49], teachers and pupils with voice disorders may limit this exchange and impede the learning process, potentially affecting learning outcomes. Teachers use their voices to present new information, answer questions, ask for participation, and evaluate pupils [49]. When a teacher suffers from a voice disorder, they may need to rely on alternative didactic strategies to transmit knowledge, such as guidelines, videos, and group activities, which may slow down the learning process and reduce learning success. Communication is the basis of any interaction process, and teachers are the main actors in designing and moderating interactions in the classroom. If oral interaction is not possible, the teaching and learning process will be limited, and learning objectives may not be achieved [50]. Moreover, voice disorders can also impact maintaining order inside the classroom because teachers cannot communicate efficiently with their pupils. Therefore, workplace vocal health promotion programs are useful strategies to empower teachers about their voice as a working tool, and how to use it safely in occupational settings and for pupils to understand the importance of voice in the learning process.
Limitations and Recommendations
Although this study provides valuable insights, several limitations need to be acknowledged. The primary limitation is the small sample size of participating teachers, which may hinder the generalization of our results to larger populations. Another limitation is the absence of measures taken during lectures, which limits the characterization of voice use in the classroom. To address this limitation, future studies can incorporate voice dosimetry measures during classroom lectures. A third limitation is the lack of noise measurements in the classrooms, which could have been used to validate the noise traffic light methodology. Furthermore, it should be noted that the dynamic microphone used for the voice recordings may not have been the most suitable option due to its dynamic SPL range response. Although we analyzed the standard deviation and distribution of SPL, the effect of the microphone on the measured variables may have introduced a systematic bias. Finally, the absence of a control group is another limitation. However, as this was a pilot study, we focused on examining the changes in the group exposed to the WVHPP. Despite these limitations, this study provides a foundation for future research to build upon and further investigate the impact of WVHPPs on voice use in the classroom.
Conclusions
In conclusion, the three-week WVHPP was found to have a significant impact on several acoustic parameters, such as the fundamental frequency and sound pressure levels. These findings highlight the potential of the WVHPP as an effective intervention for improving the vocal health of both teachers and students. However, the lack of a significant effect on cepstral peak prominence smoothed suggests that further research is needed to fully understand the impact of the WVHPP on voice quality.

