











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
More than a century ago, Chevalier Jackson conducted the first evaluation of the aerodigestive tract. As a result of technological advancements, laryngology procedures have become less invasive and more patient-friendly, with increased pain tolerance, and reduced procedure time and cost. Currently, a complete upper aerodigestive tract evaluation includes a trans-nasal flexible laryngoscopy or a rigid endoscopy under topical anesthesia, commonly using a distal-chip camera for better imaging resolution [1,2].
Despite these procedures being carried out in the office on a more regular basis, there is still controversy over whether they should be done routinely due to potential complications.
Complications that can occur during in-office procedures include vasovagal reaction, epistaxis, local anesthetic toxicity, bleeding from the lesion site, post-procedural aspiration, and laryngospasm. It is important to consider that not all outpatient clinics are prepared to handle these complications. That is why it is recommended for the office to be located near a hospital or at least less than 4 kilometers from it [2,3].
Several studies recommend that clinics should routinely perform screening protocols to detect patients who may be at risk of cardiovascular complications. Hemodynamic changes that commonly occur are elevation of blood pressure and tachycardia, and that is why monitoring of vitals during the procedure might be necessary in certain patients [4-6]. Not every patient is a candidate for an in-office procedure. Therefore, adequate patient selection is the most important step in order to achieve consistent results. The initial diagnostic physical exam can give us a reliable idea of patient tolerance; it will also give a good evaluation of patient anatomy prior to performing these procedures. In this initial examination, the surgeon´s clinical common sense regarding patient safety becomes paramount. Patient intolerance is defined as any procedure that cannot be completed due to pain, coughing, gagging, swallowing, or anxiety. To improve patient tolerance, some authors suggest premedication with lorazepam one hour before the procedure, reporting an increase of tolerance as high as 70% [2,7,8].
Awake interventions provide various benefits, notably reducing patient morbidity, which significantly enhances the treatment of laryngeal diseases in contemporary laryngology practices. Increasing awareness of these alternatives and their numerous advantages can empower laryngologists to confidently incorporate these techniques into their own practice. Having said this, it is always important to remember that in-office laryngeal procedures by no means can replace the precision and visualization of direct microlaryngoscopy for microphonosurgery
The aim of this article is to consider in-office laryngeal procedures as a better option for selective cases due to their multiple advantages.
Methods
A thematic analysis study was performed; a selection of 25 articles showed the previous and current way to perform in-office laryngeal procedures with their respective advantages and disadvantages. The analyzed literature was complemented with the main author´s experience in performing in-office procedures for over fifteen years in a private practice setting in Latin America (Mexico).
In-Office Procedures
Procedures that are performed away from the operating room (OR), in an endoscopy suite or in the office can be divided into two general groups: 1) Diagnostic and 2) Therapeutic.
Diagnostic in-office procedures:
Visualization (stroboscopy, tracheoscopy, preoperative evaluation for procedures that could potentially result in damage to the recurrent laryngeal nerve).
Cultures (in resistant laryngeal infections).
Biopsies (transoral or through working channel).
Transnasal esophagoscopy (TNE).
Therapeutic in-office procedures:
Types of Techniques for In-Office Procedures
Transoral (curved needle, forceps).
Transnasal (working channel through a flexible endoscope).
Thyrohyoid membrane.
Cricothyroid membrane.
•Submucosal.
•Midline through the airway.
Trans-Thyroid (through the cartilage).
Trans-cervical, lateral to the larynx towards the posterior cricoid region.
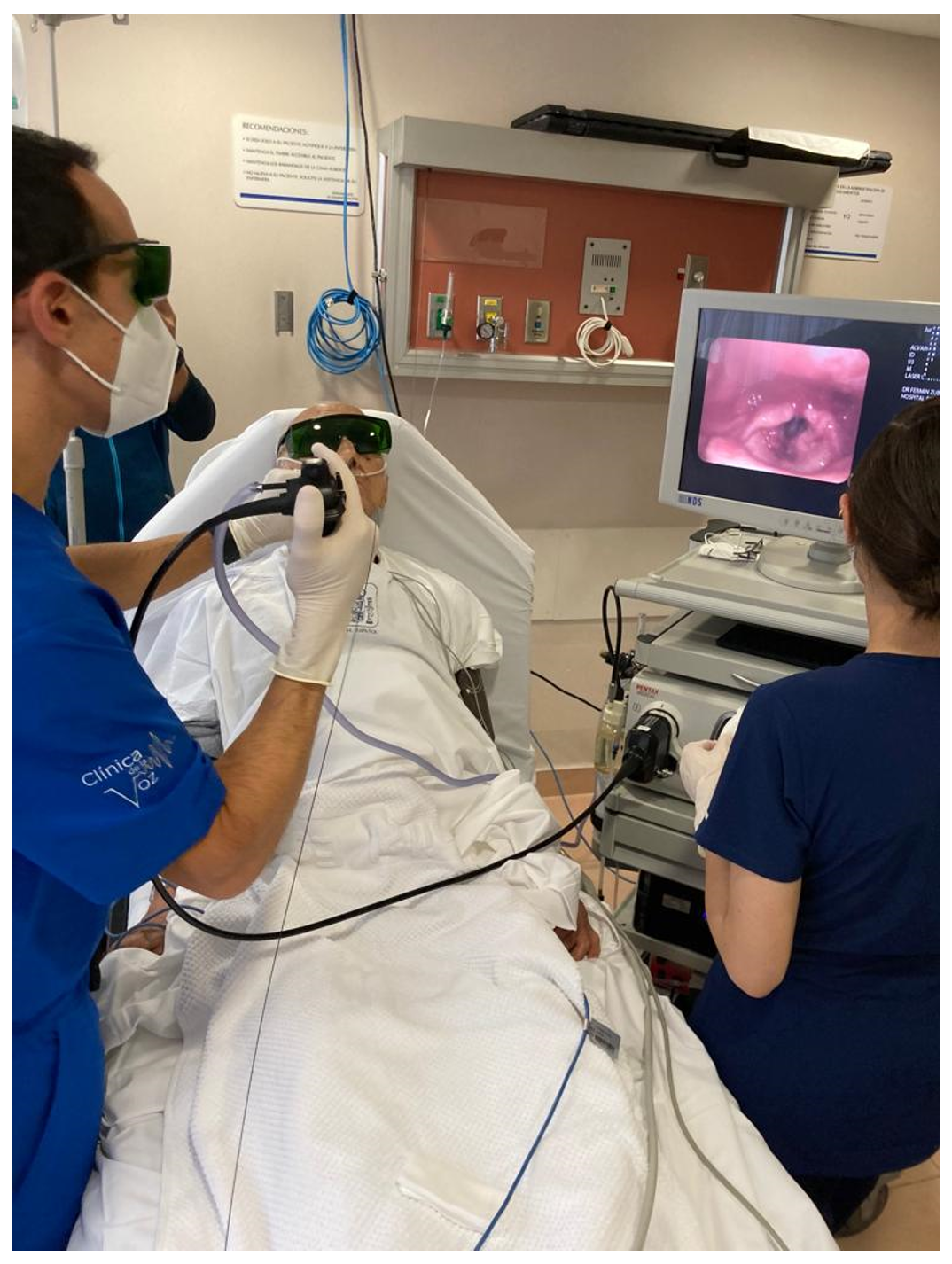
One of the most practiced office-based procedures is the biopsy of laryngeal lesions (Figure 1). Performing this procedure in the office eliminates the risks or complications that an intervention in the OR has and increases the possibility of carrying out surgical planning. This procedure is only suitable for patients with certain exophytic lesions, who have specific health risks under general anesthesia and are able to sit still with a minimal gag reflex [1].
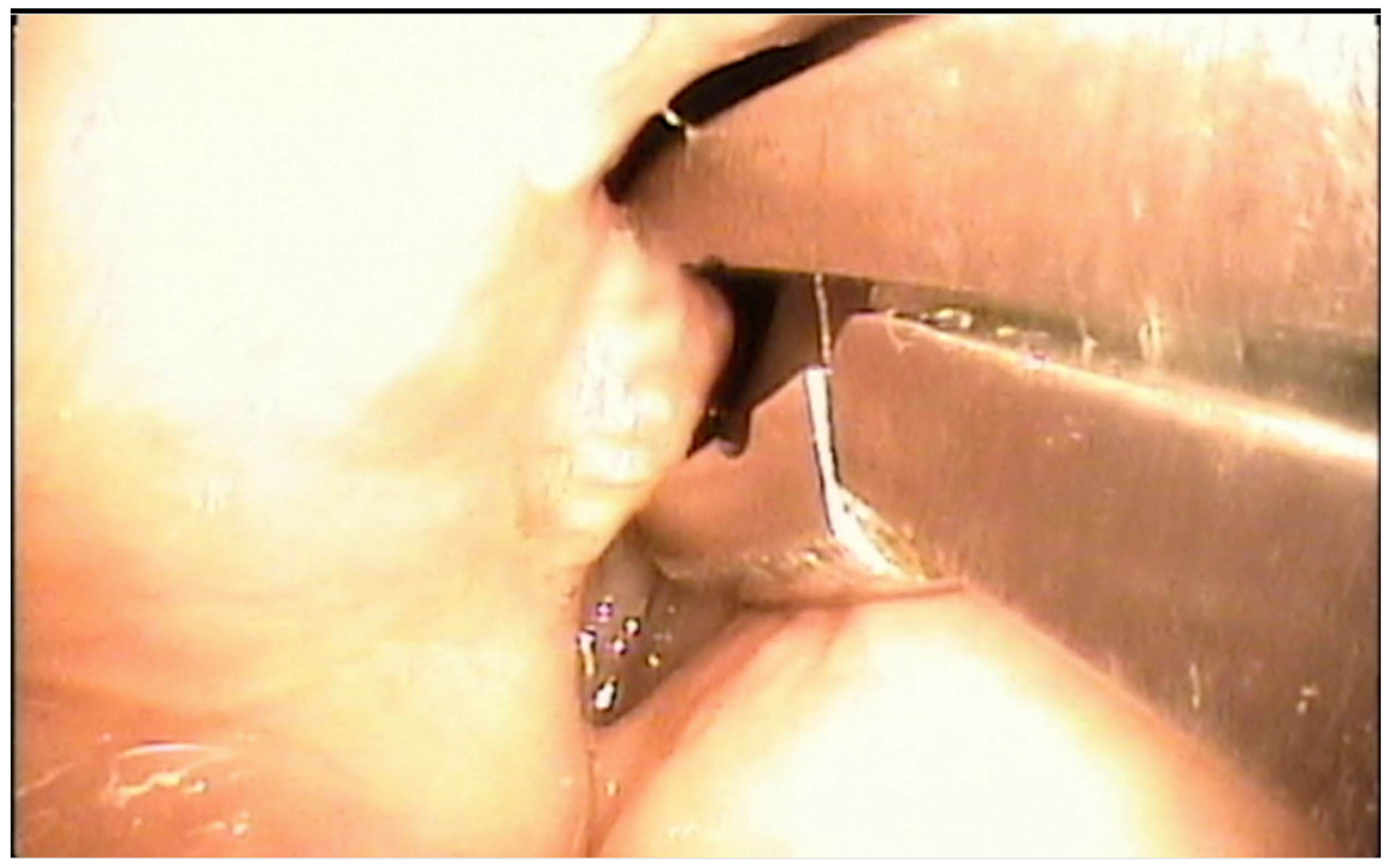
Figure 1 Biopsy of a right vocal fold tumor under local anesthesia with a transoral laryngeal forceps.
Vocal fold injection has increased in popularity and is currently one of the most widely performed in-office procedures. As mentioned above, there are multiple techniques and materials that can be injected depending on the disease being treated. Types of techniques can also be seen in Figures 2 and 3 [2].
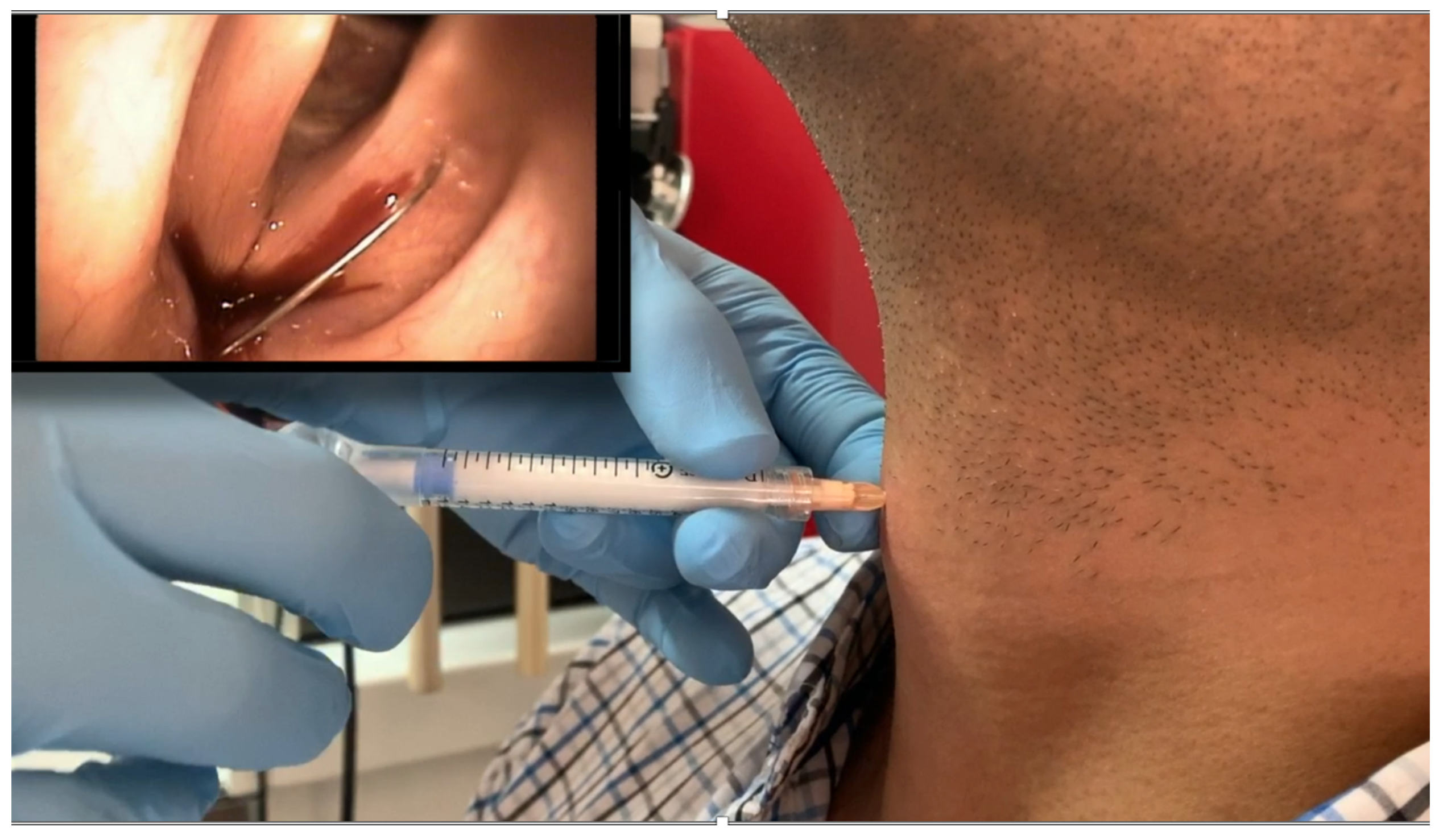
Figure 2 Injection laryngoplasty / vocal fold augmentation. Thyrohyoid membrane (Calcium Hydroxyapatite-CAHA).
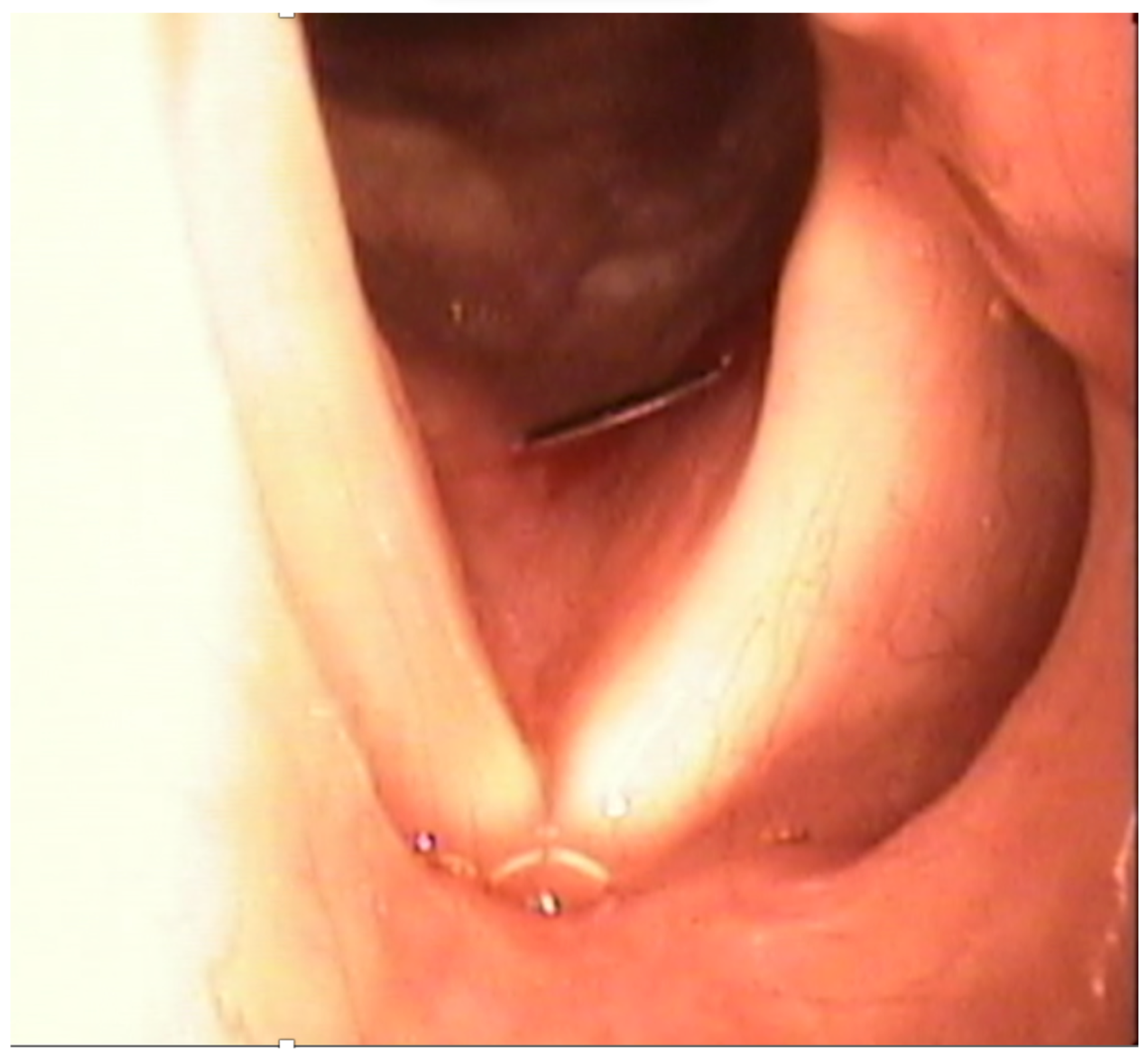
Figure 3 Injection laryngoplasty / vocal fold augmentation. Cricothyroid membrane (Hyaluronic Acid).
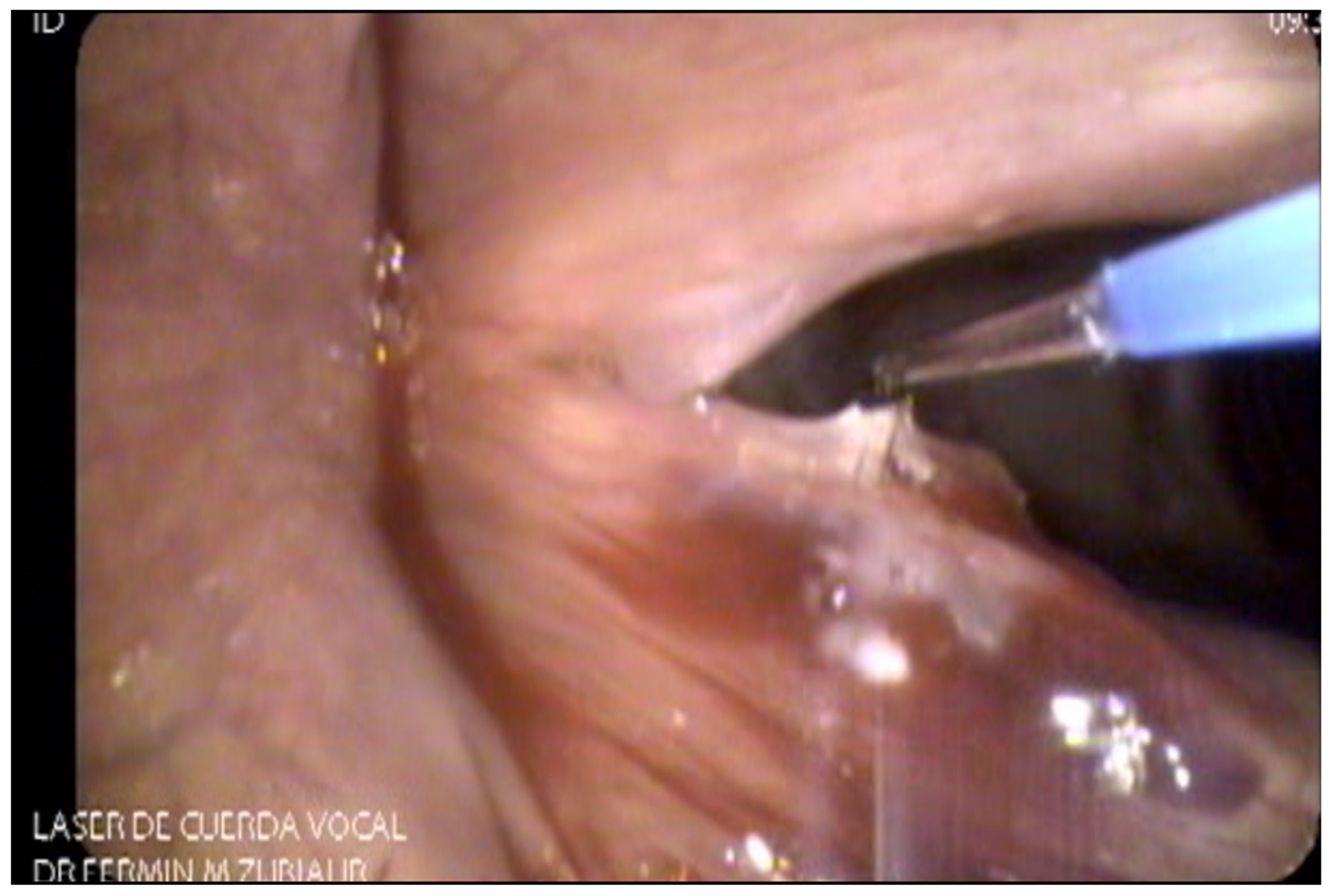
As far as lasers are concerned, [9-11] there is a wide variety of laser technology available for office-based surgery of the upper aerodigestive tract. The most commonly used laser in the history of laryngeal surgery is the CO2 laser which works in the infrared spectrum with a wavelength of 10600nm and has been used primarily in microphonosurgery. Photoangiolytic fiber-based lasers such as PDL (wavelength of 585 nm), KTP (532 nm), and TruBlue (445 nm) have dramatically changed the way laryngeal procedures are performed and have been a key factor for the popularity office-based laser procedures have gained (Figures 4, 5 and 6). Laser selection depends on availability, surgeon familiarity with each technology, and disease characteristics [7,12-18]. Office-based laser surgery has been used for the treatment of benign lesions, including polyps, exophytic phonotraumatic lesions, ectasias Reinke´s edema, stenosis, and select cases of leukoplakia and pre-malignant lesions under specific therapeutic protocols [15,19,20].

Discussion
After general anesthesia was introduced for the first time in 1846, the main way laryngeal procedures were done was through direct microlaryngoscopy in the operating room [21]. Thanks to technological advances, specifically in rigid and flexible endoscopy, in-office procedures have become a well-accepted alternative that has gained increased popularity. Fortunately, a great number of laryngeal diseases can be treated in the office or endoscopy suite with patients under superficial sedation or local anesthesia, lowering procedure time and costs compared to the operating room. The possibility of performing a procedure in an awake patient also provides efficient time management during daily activities for the surgical team with outpatient office visits, follow-ups, and operating room scheduling.
The surgical skill, technique preference and learning curve of the surgeon plays an important role when choosing the best treatment modality, but each patient´s economic situation and their private or public health insurance status is also a key factor to consider.
Most patients who have undergone some type of previous surgery in the OR feel more comfortable and safer when procedures are performed in the office [22]. Significant savings have been reported when performing certain procedures in the awake patient, not to mention that suspension laryngoscopy with its inherent risks may affect the quality of life of patients as it relates to all aspects associated with surgery, in a hospitalized patient, experiencing an OR situation [8,23]. On the other hand, in-office procedures do not replace all procedures in the OR, as one of the most significant advantages of surgery with general anesthesia is the use of binocular visualization and micro-instrumentation, which in turn result in incomparable precision [7,12,13,15,24].
A retrospective study from the Boston Medical Center compared patients who underwent in-office biopsies and biopsies in the operating room. On average, the charges for in-office biopsies were $2053.91USD per patient, while the cost for operative biopsy averaged $9024.47USD per patient. In certain cases, an office-based biopsy is equally effective compared to a biopsy taken in the operating room. However, an office-based biopsy may be too superficial and might not be representative of deeper tissues [7,25]. Andrade Filho et al. reported the difference in costs, specifically for vocal fold injections with an average cost of $1,200USD in the office compared to an average of $12,400USD in the operating room [7,26].
Health services in many countries are public or work with certain health insurances. Access to quality specialized medical treatment in public hospitals in Latin America is the norm but generally in third level/specialty based medical centers that are mostly overwhelmed with patients in the clinics and in the OR. Additionally, the need to reach a balance of adequate medical attention, while shortening waiting periods for patients, increases bureaucracy and makes opportunities for modifications in time efficiency a difficult task in most general clinics and hospitals. This might limit access to in-office procedures to only these specialized centers, while the vast majority of general medical centers and clinics are limited in trained fellowship trained professionals and/or in adequate equipment to be able to perform routine awake procedures. For many patients, this leaves the possibility of receiving quick therapeutic alternatives for in-office procedures only through specialists in the private medical care setting.
We presented the results of a survey on in-office procedures, in the most recent Panamerican Otolaryngology congress in Orlando, 2022. The survey included 18 questions and was distributed among Otolaryngologists from north, central, and south America that focus their practice mainly in laryngology or voice medicine. There was a significant difference in the number of awake procedures that are being performed in the United States, compared to most Latin American countries, where a large percentage of all laryngology related procedures and surgeries are done in the office setting, compared to only a smaller fraction of this total in Latin America. The above-mentioned factors are unmistakably a reason this is the current trend at least in the American continent.
Conclusion
Laryngology office-based procedures have become more reproducible in recent years due to the improvement in technology and endoscopic equipment as well as the increasing availability of training programs and centers. Numerous benefits are obtained with awake interventions, such as reduced procedure time and costs as well as less patient morbidity, resulting in an important way laryngeal diseases are treated in modern day laryngology practices around the world. Limitations in the way surgeons are able to train for these procedures, as well as all the bureaucratic institutional aspects of public hospitals, may all play a role as to why office-based procedures are still performed in suboptimal percentages in many countries, even when their advantages have been well demonstrated. Despite their many advantages, in-office laryngeal procedures by no means can replace the precision and visualization of direct microlaryngoscopy for microphonosurgery

