Recibido: 15/08/05 Aprobado: 01/09/05
Resumen
El síndrome metabólico (SM) es un conglomerardo de factores de riesgo, todos ellos asociados con un componente principal causante que es la adiposidad visceral y que identifica a quien lo posee con un riesgo de desarrollar enfermedad cardiovascular (ECV) o diabetes mellitus tipo 2 (DM-2). En los últimos años se ha enfatizado en este síndrome por la alta prevalencia progresiva de obesidad y DM-2 a nivel mundial. Múltiples clasificaciones se han propuesto, que dificultan homologar los estudios y resultados sobre el riesgo de enfermedad cardiovascular. Recientemente la Federación Internacional de Diabetes ha propuesto una clasificación que se espera sea la aplicada a partir de la fecha en el mundo. Esta revisión enfatizará en el riesgo de ECV asociado al SM.
]]> Palabras claves: síndrome metabólico, enfermedad cardiovascular, diabetes mellitus, glicemia anormal en ayunas, intolerancia a la glucosa, obesidad visceral, perímetro abdominal, hipertrigliceridemia, colesterol de alta densidad.Summary
Metabolic syndrome (MS) consists of a series of risk factors, all of them associated with visceral fat leading to a high risk of developing cardiovascular disease or type II diabetes mellitus. Emphasis has been made on this syndrome in recent years due to the increasingly high prevalence of obesity and type-II diabetes world wide. Multiple classifications have been proposed, making it difficult to standardize studies and outcomes regarding the risk of cardiovascular disease. The International Diabetes Federation has proposed recently a new classification which is expected to be implemented throughout the world. The purpose of this paper is to emphasize the risk of cardiovascular disease associated with metabolic syndrome.
Key words: metabolic syndrome, cardiovascular disease, diabetes mellitus, abnormal fasting glycemia, glucose intolerance, visceral obesity, waist circumference, hypertriglyceridemia, high-density cholesterol
Introducción
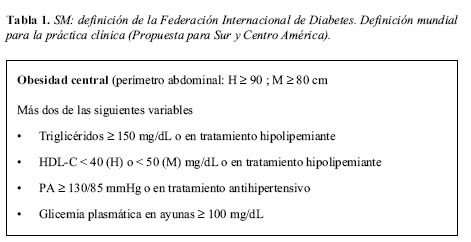
El Dr. Reaven en 1988 enfatizó con sus publicaciones, en el concepto de riesgo de ECV y diabetes en pacientes con el llamado, hoy día, SM (1). Desde entonces, múltiples clasificaciones han propuesto diferentes variables y valores para los factores de riesgo que lo componen (2-4). La clasificación más usada en nuestro medio, por lo práctica, es la del Programa Nacional de los Estados Unidos sobre Educación en Colesterol, III Panel de Tratamiento para Adultos (NCEP-ATPIII) (4). En los países europeos predomina la clasificación EGIR (3) que es una modificación de la propuesta por la Organización Mundial de la Salud (OMS) (2). La falta de unificación en la clasificación dificulta homogenizar los resultados sobre riesgo cardiovascular. Con las nuevas investigaciones sobre SM, principalmente en lo concerniente a adiposidad visceral y valores normales de glicemia, la Federación Internacional de Diabetes ha propuesto una definición, como propuesta para aplicar en la práctica clínica en forma universal y así facilitar las investigaciones (documento aún no publicado en revistas) (Tabla 1).
Importante observar que el perímetro abdominal propuesto para Sur y Centro América son los anotados en la Tabla 1. En el 2003, en Colombia, se publicó como 88 cm. el perímetro abdominal que identifica riesgo cardiovascular (5).
Síndrome metabólico, riesgo de diabetes y enfermedad cardiovascular
]]> El SM está asociado con un incremento del riesgo tanto para DM-2 (6,7), como para ECV (8-21), entendiéndose con este término, al conjunto de patologías como el infarto de miocardio (IM), angina, evento cerebrovascular (ECV), enfermedad arterial periférica, revascularización y mortalidad por estas causas. Es difícil precisar el riesgo de ECV, secundaria al SM en forma universal, por la falta de unificación en la definición escogida en el estudio, las variables utilizadas, la variabilidad en el riesgo ajustado, la población analizada, el tipo de estudio (prospectivo, corte transversal, subestudio, etc.). La mayoría de resultados pertenecen a los tres últimos años. De manera resumida se analizarán los resultados de los siguientes estudios:A. Se ha demostrado mayor porcentaje de obstrucción en las arterias coronarias en pacientes con SM (8) y este compromiso es directamente proporcional al número de componentes del SM (9).
B. Cuando se analiza morbilidad hay cinco estudios que analizan el riesgo relativo (RR) para eventos coronarios mayores (IM, angina, muerte súbita), ECV, enfermedad coronaria (IM, angina, revascularización, isquemia). La Figura 1 esquematiza los RR. En un subestudio del 4S y del AFCAPS/TexCAPS, de los pacientes con síndrome metabólico, a cinco años y utilizando la clasificación del NCEP-ATPIII, el RR en general fue de 1.5 para eventos coronarios mayores, IM fatal y no fatal o ECV, con intervalos de confianza que hacen significativos sus resultados (10).
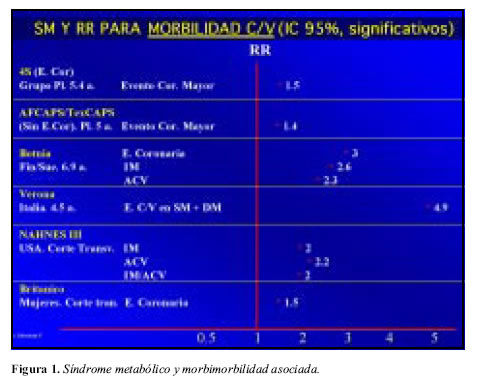
Resultados similares utilizando la clasificación de la OMS, muestra el estudio Botnia en población filandesa y Suiza (11). El RR para enfermedad coronaria (EC), IM, ECV encontrado fue de 3, 2.6 y 2.3 respectivamente en un seguimiento a siete años y todos con valor de p significativo. El RR para mortalidad cardiovascular fue de 1.8, igualmente significativo. En el estudio Nhanes III (12), el RR para IM o ECV aislados o para la asociación IM/ECV, es de aproximadamente dos, con IC95% significativos, utilizando la definición del NCEP. El alto riesgo de ECV en el diabético que además presenta SM, lo muestra el estudio Verona Diabetes Complications (13), que encuentra un RR significativo de 4.9 (p=0.03) con la asociación SM + DM. En mujeres, el Estudio Británico del Corazón y la Salud (14), demostró un RR (IC95%) de 1.53 (1.3-1.9) para enfermedad coronaria (IM, angina). Este riesgo fue similar utilizando la clasificación de la NCEP u OMS y para la glicemia > 100 mg/dL, HDL< 40 mg/dL, triglicéridos (TG) > 150 mg/dL o cintura > 88 cm (Figura 1).
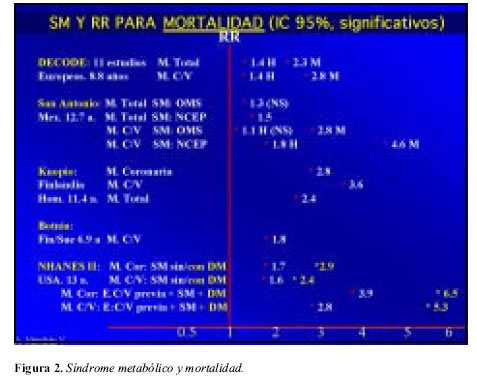
C. Cuando se analiza el RR para mortalidad de origen coronario, cardiovascular o total, secundaria al SM, hay cinco estudios que se resumen en la Figura 2. El estudio Decode (15) es un importante metaanálisis de 11 estudios de cohortes, prospectivos, de Europa (posiblemente el único metaanálisis a la fecha sobre SM), que aplicaron la clasificación modificada de la OMS (EGIR), con seguimiento a 8.8 años, y que incluyó 6.156 hombres y 5.356 mujeres. El grupo con SM, mostró un RR (IC95%) para mortalidad total de 1.4 (1.2-1.8) para hombres y de 2.3 (1.6-3.2) para mujeres. Similar comportamiento se observó para mortalidad cardiovascular. Demuestra este estudio que el SM en mujeres tiene un riesgo mayor de mortalidad que en hombres. Datos similares del comportamiento del SM en mujeres lo aporta el Estudio del Corazón de San Antonio (Texas) (16), que incluyó un alto porcentaje de mexicanos. En este análisis el RR (IC95%) para mortalidad cardiovascular en mujeres con SM fue de 4.6 (2.4-9.2) y de 1.8 (1.1-2.9) para hombres, cuando se aplicó la clasificación del NCEP-ATPIII y menor el RR cuando se aplicó la clasificación de la OMS. Se dedujo de este análisis que la clasificación del NCEP-ATPIII es más predictiva y aplicable (16). El estudio prospectivo a 11 años de la Dra. Lakka HM, realizado en 1.209 hombres finlandeses (17), demostró en el grupo con SM un RR (IC 95%), del 3.8 (1.7-8.2) para mortalidad por enfermedad coronaria, un RR de 3.6 (1.2-6.4) para mortalidad por ECV y un RR de 2.43 (1.6-3.6) para mortalidad por todas las causas. En el estudio Botnia (11), el RR para mortalidad cardiovascular fue de 1.8, igualmente significativo. El estudio Nhanes II (18), analiza mortalidad y encuentra un RR (IC 95%) para mortalidad coronaria, cardiovascular y total de 1.7 (1.1-2.5), 1.6 (1.2-2.1), 1.2 (NS) respectivamente, en el grupo con SM y sin DM-2; pero al asociarse el SM a la DM-2, este RR es superior en todas las causas de mortalidad y si se asocia SM, DM-2 y ECV previa, el RR aumenta aún más y significativamente hasta seis para mortalidad por enfermedad coronaria y 5.3 para mortalidad cardiovascular. Este hallazgo enseña que el SM asociado a DM-2 o previa ECV es de peor pronóstico y que por lo tanto se debe ser más agresivo con las metas, por ejemplo LDL-c<70mg/dL (Figura 2).
D. Aunque el riesgo de eventos cardiovasculares se ha asociado con la presencia del SM, también se ha demostrado que la glicemia anormal o la intolerancia a la glucosa, también tienen riesgo para ECV. Este riesgo lo demuestra un metaanálisis de 38 estudios prospectivos (19). Con niveles de glicemia en ayunas entre 97 y 130 mg/dL comparado con el nivel más bajo entre 66 y 90 mg/dL, el RR (IC 95%) para ECV es de 1.27 (1.13-1.43). Con valores de glicemia después de una prueba de tolerancia a la glucosa oral (poscarga) entre 150 y 194 comparado con 69 a 107 mg/dL, el RR (IC95%) para ECV fue de 1.27 (1.1-1.48) (19).
]]> E. El engrosamiento íntima-media de las arterias carótidas ha sido mostrado indirectamente como predictor de enfermedad coronaria como lo demuestra el estudio ARIC en personas con SM (20). Igualmente la obesidad abdominal se ha asociado con el diámetro de la luz coronaria (21).Cálculo del riesgo de evento coronario a 10 años para el síndrome metabólico, de acuerdo con las tablas de Framingham
En forma práctica y aplicable, se puede extractar de los estudios sobre riesgo cardiovascular en el SM, las siguientes conclusiones:
A. El RR de eventos coronarios (IM, angina, revascularización) es significativo entre 1.5 y 2 cuando se encuentra el SM en forma aislada, en personas mayores de 50 años y a 8-11 años.
B. El RR para mortalidad por enfermedad coronaria se encuentra entre dos y tres ante la presencia de SM en forma aislada; sin embargo, el RR para mortalidad cardiovascular o coronaria puede estar entre cinco y seis respectivamente, cuando se asocia al SM, la diabetes mellitus o la enfermedad cardiovascular previa.
Hablar de riesgo relativo es útil, pero es más predecible y entendible para el médico o el paciente, referirse al riesgo de eventos coronarios (infarto del miocardio o muerte de origen coronario) a 10 años y expresar este riesgo con valores menores a 10%, entre 10 y 20% o mayor a 20%. Si se utilizaran las tablas de Framingham para un paciente con SM aislado, es decir, que no se asocie el SM a DM o ECV previa (casos que por definición tienen un riesgo a 10 años mayor a 20%), es posible que el riesgo calculado sea menor a 10%. Esto se explica por no estar dentro de las variables para Framingham el perímetro abdominal o la obesidad, los triglicéridos y las alteraciones de la glicemia en rangos no diabéticos. De otra parte el riesgo de eventos coronarios en las tablas de Framingham van a la par con la edad del paciente y sólo con edades mayores de 50 años en hombres y 60 años en mujeres el riesgo de eventos coronarios empiezan a ser mayores a 10% (22). Por ello en hombres menores a 50 años y mujeres menores a 60 años, no fumadores y sin hipercolesterolemia severa, que tengan SM aislado, el riesgo a 10 años propuesto debe estar entre 10 y 20%, sin necesidad de aplicar las tablas, pues si se utilizaran, el riesgo sería menor a 10%. Recientemente se le ha dado importancia a la PCR-hs, para valorar riesgo cardiovascular en el SM (23-26).
Posibles explicaciones a la asociación SM y enfermedad cardiovascular
Son múltiples las teorías propuestas para explicar la ECV y DM-2 asociadas con el SM. Se sabe que cada uno de los componentes del SM es un factor de riesgo para ECV. Se ha implicado al adipocito visceral y a la resistencia a la insulina como los causantes, aunque para algunos es una manera simplista de explicar la situación. El adipocito visceral al liberar factor de necrosis tumoral alfa, IL-6 (manifestando PCR-hs), PAI-1, resistina, adiponectina baja y altos niveles de ácidos grasos libres, predispone a la dislipidemia aterogénica, hipertensión arterial, "ateroscleritis", disfunción endotelial, resistencia a la insulina (disglicemia e hipertrigliceridemia) y estado protrombótico. Algunas de las revisiones sobre el tema se anexan en la bibliografía (27-31).
Tratamiento del síndrome metabólico
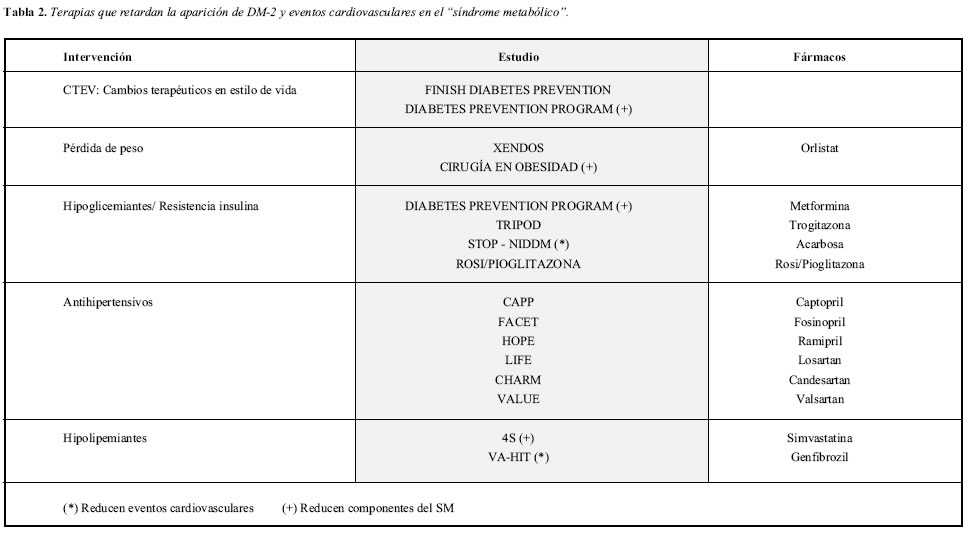
El tratamiento actual óptimo para disminuir las complicaciones del SM (ECV y DM-2), es con la intervención multifactorial, simultánea y buscando metas, de cada uno de los componentes del SM. La Tabla 2 resume las diferentes intervenciones que han mostrado primordialmente retardo en la aparición de DM-2 de novo (32-37). La regresión de casi todos los componentes del SM se ha logrado con cambios terapéuticos en estilo de vida (CTEV) (38) y con cirugía para obesidad (39). La disminución del riesgo de ECV en SM se ha demostrado con estatinas (40), fibratos (41) y con acarbosa (42), aunque la evidencia es derivada de estudios clínicos posteriores. Con acarbosa se ha demostrado reducción del riesgo de IM e hipertensión en obesos con intolerancia a la glucosa (ITG) (42). La recomendación fundamental es insistir en los CTEV (32, 33). Al momento no hay suficiente evidencia para recomendar universalmente tiazoledinedionas (35, 36), metformina (33, 38), acarbosa (34, 42) u orlistat (37) para retardar la DM-2 o para disminuir el riesgo de ECV, aunque su uso podría estar indicado en algunos casos y dependiente del criterio médico, principalmente en personas que no se adhieren a los CTEV. La aspirina debe estar en todos los pacientes, si no hay contraindicación. El clopidogrel es otra alternativa. Se esperan resultados clínicos con el uso de bloqueadores de receptores de canabinoides CB1 (rimonabant), los cuales regulan los factores de riesgo asociados con el exceso de grasa visceral.
]]> ConclusionesEl SM ha demostrado ser un riesgo para DM-2 y ECV. El riesgo para ECV es aún más alto cuando se asocia el SM a DM-2 y/o a ECV previa.
Con SM, al utilizar las tablas de Framingham, el riesgo de eventos coronarios a 10 años en personas mayores de 50 años no fumadoras, suele ser de 10-20%. Cuando se tiene más de 50 años, fumador e hipercolesterolémico severo es posible que este riesgo sea mayor a 20%. Por el contrario en menores de 50 años no fumadores pero con SM, el riesgo a 10 años calculado con las tablas, puede ser menor a 10%, caso en el cual se debe ignorar las tablas y predecir el riesgo entre 10 y 20%. Se debe insistir en la prevención de la aparición del SM mediante CTEV. En personas con SM, los CTEV son el pilar del tratamiento. Los fármacos como la metformia, tiazoledinedionas, acarbosa y el orlistat, podrían ser útiles en algunas situaciones para prevenir o retardar la aparición de DM-2 o ECV, aunque su evidencia no está completamente aceptada. Las estatinas y los fibratos han demostrado beneficio en SM y posiblemente el ácido nicotínico o estos hipolipemiantes asociados, son benéficos pero de acuerdo con el perfil lipídico en particular.
Bibliografía
1. Reaven GM. Role of insulin resistance in human disease. Diabetes 1988;37:1595-1607. [ Links ]
2. Alberti KG, Zimmet PZ, for the WHO Consultation. Definition, diagnosis and classification of Diabetes Mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus. Report of a WHO consultation. Diabet Med 1998;15:539-553. [ Links ]
3. EGIR. European Group for Insulin Resistance. Diabet Med 1999;16:442. [ Links ]
4. Executive Summary of The Third Report of the National Cholesterol Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497. [ Links ]
5. Perez M, Casas JP, Cubillos LA, Serrano NC, Morillo C, Lopez-Jaramillo P. Utility of the waist circunference as screening tool to identify Colombian subjects at cardiovascular risk. Eur J Cardiovasc Prev Rehabil 2003;10:328-335. [ Links ]
6. Hanson RL, Imperatore G, et al. Components of the metabolic syndrome and incidence of type 2 diabetes. Diabetes 2002;51:3120-3127. [ Links ]
7. Laaksonen DE, Lakka H-M, Niskanen LK, Kaplan GA, Salonen JT, Lakka TA. Metabolic Syndrome and development of diabetes mellitus: Application and validation of recently suggested definitions of the metabolic syndrome in a prospective cohort. Am J Epidemiol 2002;156:1070-1077. [ Links ]
8. Solymoss BC, Bourassa MG, Lesperance J, et al. Incidence and clinical characteristics of the metabolic syndrome in patients with coronary artery disease. Coronary Artery Disease 2003;14:207-212. [ Links ]
9. Solymoss BC, Bourassa MG, Campeau L, et al. Effect of increasing metabolic syndrome score on atherosclerotic risk profile and coronary artery disease angiographic severity. Am J Cardiol 2004;93:159-164. [ Links ]
10. Girman CJ, Rhodes T, Mercuri M, et al. The metabolic syndrome and risk of major coronary events in the Scandinavian simvastatin survival study (4S) and the Air Force/Texas coronary atherosclerosis prevention study (AFCAPS/TexCAPS. Am J Cardiol 2004;93:136-141. [ Links ]
11. Isomaa B, Almgren P, Tuomi T, Forsén,B, Lahti K, Nissén M, Taskinen M-R, Groop L. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001;24:683-689. [ Links ]
12. Ninomiya JK, L'Italien G, Criqui MH, et al. Association of the metabolic síndrome with story of myocardial infarction and stroke in the III National Health and Nutrition Examination Survey. Circulation 2004;109:42-46. [ Links ]
13. Bonora E, Targher G, Formentini G, et al. The metabolic syndrome is an independent predictor of cardiovascular disease in type 2 diabetetic subjects. Prospective data from the Verona diabetes complications study. Diabet Med 2004;21:52-58. [ Links ]
14. Lawlor S, Ebrahim, Smith GD. The metabolic syndrome and coronary heart disease in older women: findings from the British Womens Heart and Health study. Diabet Med 2004;21:906-913. [ Links ]
15. Hu G, Qiao Q, Tuomilehto J, et al. Prevalence of the metabolic syndrome and its relation to all cause and cardiovascular mortality in nondiabetic European men and women. Arch Intern Med 2004;164:1066-1076. [ Links ]
16. Hunt KJ, Resendez RG,Williams K, Haffner SM, Stern MP. National Cholesterol Education Program versus World Health Organization metabolic syndrome in relation to all cause and cardiovascular mortality in the San Antonio Heart Study. Circulation 2004;110:1251-1257. [ Links ]
17. Lakka HM, Laaksonen DE, Lakka TA, Niskanen LK, Kumpusalo E, Tuomilehto J, Salonen JT. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA. 2002;288:2709-2716. [ Links ]
18. Malik S, Wong ND, Franklin SS, et al. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in USA adults. Circulation 2004;110:1245-1250. [ Links ]
19. Levitan EB, Song Yiqing, Ford ES, et al. Is nondiabetic hyperglycemia a risk factor for cardiovascular disease? Arch Intern Med 2004;164:2147-2155. [ Links ]
20. McNeil AM, Rosamond WD, Girman CJ, et al. Prevalence of coronary heart disease and carotid arterial thickening in patients with the metabolic syndrome (The Aric Study). Am J Cardiol 2004;94:1249-1254. [ Links ]
21. Silva FA, Lopez-Jaramillo P, Casas JP, et al. Abdominal obesity is associated with coronary luminar diameter in patients with chest pain. Diabetes and Metabolism 2002;29:4sO. [ Links ]
22. Pasternak RC, Abrams J, Greenland P, et al. Identification of coronary heart disease risk. Is there a detection gap? J Am Coll Cardiol 2003;41:1863-1874. [ Links ]
23. Ridker PM, Wilson PWF, Grundy SM. Should PCR be added to metabolic syndrome and to assessment of global cardiovascular risk? Circulation 2004;109:2818-2825. [ Links ]
24. Ridker PM, Buring JE, Cook NR, et al. PCR, the metabolic syndrome, and risk of incident cardiovascular events. Circulation 2003;107:391-397. [ Links ]
25. Rutter MK, Meigs JB, Sullivan LM, et al. PCR, the metabolic syndrome and prediction of cardiovascular events in the Framingham offspring study. Circulation 2004;110:380-385. [ Links ]
26. Malik S, Wong ND, Franklin S, et al. Cardiovascular disease in US patients with metabolic syndrome, diabetes and elevated PCR. Diab Care 2005;28:690-93 [ Links ]
27. López-Jaramillo P, Siva S, Ramírez F, et al. Sindrome metabólico:diagnóstico y tratamiento. Acta Med Colomb 2004;29:137-144. [ Links ]
28. Marquez-Salom G. Obesidad e impacto cardiovascular. Acta Med Colomb 2004;29:144-149. [ Links ]
29. Miranda PJ, DeFronzo RA, Califf RM, et al. Metabolic síndrome:definition, pathophysiology and mecanisms. Am Heart J 2005;149:33-45. [ Links ]
30. Rosenson RS. New approaches in the intensive management of cardiovascular risk in the metabolic syndrome. Curr Probl Cardiol 2005;30:241-280. [ Links ]
31. Carr DB, Utzschneider KM, Hull RI, et al. Intra-abdominal fat is a major determinant of the NCEP-ATPIII criteria for the metabolic syndrome. Diabetes 2004;53:2087-2094. [ Links ]
32. Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. New Engl J Med 2001;344:1343-1350. [ Links ]
33. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346:393-403. [ Links ]
34. Chiason JL, Josse RG, Gomis R, et al. The STOP-NIDDM Trial Research Group. Acarbose for prevention of type 2 diabetes mellitus. Lancet 2002;359:2072-2077. [ Links ]
35. Buchanan TA, Xiang AH, Peters RK, et al. Preservation of pancreatic beta-cell function and prevention of type 2 diabetes by pharmacological treatment of insulin resistance in high risk Hispanic-women. Diabetes 2002;51:2796-2803. [ Links ]
36. Durbin RJ. Thiazoledinedione therapy in the prevention/delay of type 2 diabetes in patients with impaired glucose tolerance and insulin resistance. Diabetes, Obesity and Metabolism 2004;6:280-285. [ Links ]
37. Torgerson JS, Hauptman J, Boldrin MN, et al. Xenical in the prevention of diabetes in obese subjects (XENDOS) study. A randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care 2004;27:155-161. [ Links ]
38. The diabetes Prevention Program Research Group. Impact of intensive lifestyle and metformin therapy on cardiovascular disease risk factors in the diabetes Prevention Program. Diabetes Care 2005;28:888-894. [ Links ]
39. Lee W, Huang MT, Wang W, et al. Effects of obesity surgery on the metabolic syndrome. Arch Surg 2004;139:1088-1092. [ Links ]
40. Pyorala K, Ballantyne C, Gumbiner B, Lee MW, Shah A, Davies MJ, Mitchel YB, Pedersen TR, Kjekshus J for the Scandinavian Simvastatin Survival Study Group. Reduction of cardiovascular events by simvastatin in nondiabetic coronary heart disease patients with and without the metabolic syndrome. Diabetes Care 2004; 27:1735-1740. [ Links ]
41. Robins SJ, Rubins HB, Faas FH. (VA-HIT). Insulin resistance and cardiovascular events with low HDL cholesterol. Diabetes Care 2003;26:1513-1517. [ Links ]
42. Chiasson JL, Josse RG, Gomis R, et al. Acarbose treatment and the risk of cardiovascular disease and hypertension in patients with impaired glucose tolerance. The STOP-NIDDDM trial. JAMA 2003;290:486-494. [ Links ] ]]>
{kind=link}