Análisis de polimorfismos APO-E en mujeres colombianas con osteoporosis y correlación con variables clínicas y sociales de riesgo
Elsa Villarreal 1 , Antonio Bermúdez 2
1 Grupo de Nutrición, Instituto Nacional de Salud, Bogotá, D.C., Colombia.
2
Grupo de Genética, Instituto Nacional de Salud, Bogotá, D.C., Colombia.Varios estudios han demostrado la asociación de los polimorfismos de la apolipoproteína E (APO-E) con la osteoporosis, especialmente, la APO-E 4. Para analizar los polimorfismos APOE e identificar la asociación con variables clínicas y sociales, se realizó un estudio descriptivo de 32 mujeres con osteoporosis, provenientes de diferentes regiones de Colombia, mediante metodologías PCR y RFLP.
Se observaron en osteoporosis, osteopenia y osteoporosis combinada con osteopenia frecuencias para el genotipo
e 3/e3 en el 84,3% (n=27), y en el 15,6% para los genotipos con el alelo e4 (e3/e4=12,5%, n=4; e4/e4=3,1%, n=1); la misma tendencia se observó en la distribución por edad de la menopausia, e3/e3 en el 83,3% (n=25), y genotipos con el alelo e4 en el 16,6% (n=5) (e3/e4=13,3%, n=4; e4/e4=3,3%, n=1). No hubo asociación de APO-E4 con estrato socioeconómico, fracturas, enfermedades o consumo de lácteos.Aunque no hubo efecto del alelo
e4 en la densidad mineral ósea (DMO) de la columna lumbar: e4+/-(e3/e4 0,960±0,144 g/cm2); e4+/+ (e4/e4 0,873±0,00 g/cm2); e4-/- (e3/e3 0,858±0,160 g/cm2); p=0,49, ni en cuello femoral: e4+/-(e3/e4 0,841±0,026 g/cm2); e4+/+ (e4/e4 0,842±0,00 g/cm2); e4- /- (e3/e3 0,735±0,013 g/cm2), p=0,14, al explorar las diferencias de medias de DMO en el cuello femoral, se observó una diferencia significativa, t=4,17 p=0,05.Estos datos confirman una frecuencia del alelo e4 similar a lo reportado en poblaciones caucásicas y japonesas; se sugiere realizar estudios a gran escala para esclarecer el impacto de la APO-E sobre la DMO y su relación dosis-efecto.
Palabras claves: apolipoproteína E, polimorfismos, genotipos, osteoporosis, DMO, alelo.
]]> Polymorphismsof APO-E in Colombian women with osteoporosis: correlation among clinical and s9ocial risk variablesSeveral studies have reported an association between apolipoprotein E polymorphisms and osteoporosis, specially the genotype APO-E4.
In order to analyze the APO-E polymorphisms and to identify their association with clinical and social variables, a descriptive study was undertaken that included 32 women with osteoporosis, from different regions of Colombia. The polymorphisms were detected by PCR and RFLP methods.
In osteopenia and osteoporosis combined with osteopenia were observed the genotype
e3/e3 in the 84% (n=27), and 16% (e3/e4=12,5%, n=4; e4/e4=3,1%, n=1) for the genotypes bearing the e4 allele. The same tendency was observed by age of the menopause, e3/e3 in the 83% (n=25), and the genotypes bearing the e4 allele in the 17% (n=5)(e3/e4=13,3%, n=4; e4/e4=3,3%, n=1). No association of APO-E4 was detected with socioeconomic stratum, fracture, illness, surgeries, and milk consumption.No significant differences were observed in the bone mineral density (BMD) of the lumbar column between the genotypes with or without the
e4 allele e4+/- (e3/(e 4 0.96±0.14 g/cm2); (e 4+/+ ((e 4/(e 4 0.87±0.0 g/cm2); (e 4-/- ((e 3/(e 3 0.86±0.16 g/cm2); p=0.49, and femoral bone mineral density (e 4+/- ((e 3/(e 4 0.84±0.03 g/cm2); (e 4+/+ ((e 4/(e 4 0.84±0.0 g/cm2); (e 4-/- ((e 3/(e 3 0.74±0.01 g/cm2); p=0.014.However, when exploring the differences of BMD in the femoral neck, a significant difference was observed (t=4.17, p=0.05).
These results confirm e4 allele frequencies similar to those reported for caucasian and Japanese, subjects. Larger studies are necessary to elucidate the effect of APO-E in bone marrow and the dose-effect relation.
Key words: apolipoprotein E, polymorphisms, genotype, osteoporosis, allele, BMD.
La osteoporosis es una enfermedad metabólica con un fuerte componente genético (1); la asociación de polimorfismos de varios genes con la pérdida de masa ósea y el riesgo de sufrir fracturas han contribuido a predecir la condición del hueso y a esclarecer los mecanismos de la pérdida de masa ósea en esta enfermedad (2-5); la modulación genética unida a factores hormonales, dieta y estilo de vida podrían tener alguna influencia en la regulación y arquitectura del hueso.
La asociación de los polimorfismos de la apolipoproteína E (APO-E) con el metabolismo mineral óseo, particularmente la isoforma APO-E 4, ha sido demostrada por el excesivo catabolismo de la vitamina K que actúa como cofactor en la formación de residuos g carboxiglutamato de la osteocalcina, proteína de la matriz del hueso que se une al calcio (4,6,7). La vitamina K parece ejercer una inhibición parcial de la absorción del calcio en los osteoblastos al reducir la apoptosis innecesaria en estas células (8,9).
]]> El efecto del estado nutricional y metabólico es determinante en la biodisponibilidad y en el equilibrio del calcio en el organismo; los productos lácteos como la lactosa, la caseína y el citrato de calcio, entre otros, contribuyen a incrementar la retención de calcio; otras sustancias como los glucocorticoides, el alcohol y el cigarrillo disminuyen su absorción y ejercen un efecto negativo en el sostenimiento de la masa ósea.En Colombia se han realizado estudios desde la perspectiva de descripción de casos, frecuencias institucionales, ensayos clínicos de medicamentos, evaluación de métodos diagnósticos como densitometría ósea y estudios de prevalencia, de los cuales el mejor documentado es el de la Prevalencia de la osteoporosis en Santafé de Bogotá; de acuerdo con este estudio, la osteoporosis es un problema de salud pública por cuanto la prevalencia promedio es del 57% en población mayor de 40 años (10); este hallazgo llevó a la organización de un Programa de Vigilancia Centinela de la Osteoporosis según criterios de la Organización Mundial de Salud (OMS) (11), y a la búsqueda de la susceptibilidad genética que facilite la ejecución de programas de promoción y prevención de la enfermedad. Los marcadores genéticos como el gen APO-E, que se correlaciona con la densidad mineral ósea, podrían ser de ayuda para predecir y esclarecer los mecanismos de pérdida de hueso en la osteoporosis; su importancia radica en que permitiría diagnosticar a tiempo la enfermedad para tomar medidas preventivas.
El objetivo de este estudio fue analizar los polimorfismos APO-E en mujeres con osteoporosis y relacionarlos con variables clínicas y sociales para identificar su importancia en la frecuencia de la enfermedad.
Materiales y métodos
De la muestra de 50 individuos detectados en el programa de vigilancia centinela de la osteoporosis según criterios de la Organización Mundial de la Salud (11), 48 eran mujeres y sólo 32 tenían la información completa del cuestionario sobre costumbres, factores de riesgo, estrato socioeconómico, educación, edad de inicio de la menopausia, antecedentes de fracturas, cirugía, enfermedades y consumo de lácteos (leche, queso duro y blando); además, cumplían con los criterios de inclusión: densidad mineral ósea inferior a una desviación estándar, definida como diagnóstico por el método de absorciometría de fotón dual.
Las 32 mujeres estaban en un rango de edad de 30 a 82 años y provenían de diferentes regiones del país. La mayoría había realizado estudios de primaria y secundaria y pertenecía a los estratos 2 y 4 (
cuadro 1); algunas manifestaron haber sufrido fracturas, problemas de tensión, de tiroides y diabetes.
Se obtuvieron muestras de sangre con EDTA de cada paciente para la extracción del AND genómico por el método salino (12). La tipificación del gen APO-E se realizó según la modificación del protocolo de Crock (13) y se utilizaron los iniciadores del protocolo de Wenham (14).
Para la amplificación del gen, se utilizaron 200 ng de ADN en un volumen total de 25 ml con las siguientes condiciones: iniciadores APO-A y APOB 0, 2 mM, DMSO 100%, MgCl2 2,5 mM, dNTP 0,2 mM y Taq polimerasa 0,1 U/ml.
]]> Las condiciones de la amplificación fueron: predesnaturación a 94°C, 10 min; desnaturación a 94°C, 30 s, cuarenta ciclos; apareamiento a 65°C, 30 s, cuarenta ciclos; polimerización a 72°C, 30 s, cuarenta ciclos; pospolimerización a 70°C, 10 min, cuarenta ciclos.El producto amplificado se visualizó por electroforesis en agarosa al 2% y se digirió con HhaI 1 U/ml, durante 18 horas a 37°C en baño María; los fragmentos obtenidos se visualizaron por electroforesis en gel de poliacrilamida al 20%; se compararon los tamaños con un marcador de peso molecular conocido
fX 174 con enzima Hinf III y controles de pacientes ( figura 1).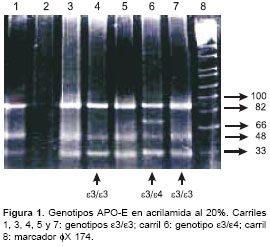
Análisis estadísticos
Se realizó el análisis de las frecuencias de alelos y genotipos por conteo de los alelos. Para correlacionar los polimorfismos con las variables clínicas, se utilizó la base de datos Epi-Info 6.04, aplicando la prueba de la ji al cuadrado. La diferencia entre la densidad mineral ósea en la columna lumbar y en el cuello femoral con cada genotipo se realizó por Anova, por medio de la prueba de Fisher y se obtuvo el valor Z al normalizar cada dato para observar diferencias entre la densidad mineral ósea de los genotipos con el alelo
e4 y sin él y se aplicó la prueba de ji al cuadrado. Se aplicó la prueba t de Student para las diferencias de medias en densidad mineral ósea de columna lumbar y cuello femoral; un valor de p< 0,05 se consideró estadísticamente significativo.Resultados
Las 32 mujeres estaban en un rango de edad de 30 a 82 años; el decil de 60 a 69 años (37,5%) fue el más frecuente; el 78% (n=25) provenía de diferentes regiones del país y el 22% (n=7) de Bogotá. La mayoría pertenecía a los estratos 2 (28,2%) y 4 (28,2%); realizaron estudios de primaria y secundaria el 34,4%; para el 81,3% (n=26), su ocupación era el hogar.
La distribución de los genotipos según la edad de inicio de la menopausia se hizo con 30 mujeres que tenían esta información; el genotipo e3/e3 mostró una frecuencia del 83,3% (n=25) superior a los genotipos con el alelo e4 (
e3/e4, 13,3%, n=4; e4/e4, 3,3%, n=1) en todos los rangos de edad; no se observó diferencia estadísticamente significativa al comparar los grupos de edad con los diferentes genotipos (cuadro 2). ]]>
De las ocho pacientes que presentaron fractura, seis tenían el genotipo e3/e3 (75%) y dos pacientes (25%) presentaron genotipos con el alelo
e4 (e3/ e4=1; e4/e4=1).De las pacientes que reportaron antecedentes de enfermedades, ocho presentaron hiperglicemia, siete con el genotipo
e 3/ e 3 (85%) y una (15%) con el alelo e 4 (e 3/ e 4=1); la misma tendencia se observó en las que tenían antecedentes de hipertensión.Según la condición ósea (osteoporosis: DMSO <2,5 desviación estándar; osteopenia: DMSO entre 1 y 2,5 desviaciones estándar; se observó que el genotipo
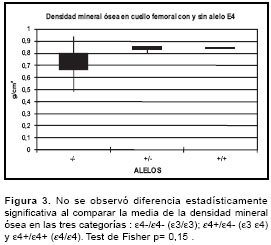
e 3/ e 3 (83,3%, n=25) fue el más frecuente en las tres condiciones óseas; los genotipos con el alelo e4 fueron menos frecuentes en el 16,6% (e 3/ e 4, 13,3%,n=4; e 4/ e 4, 3,3%,n=1), p>0,05, aunque no hubo diferencias significativas en las frecuencias de los genotipos con el alelo e4 y sin él, es importante la presencia de homocigocidad para este alelo en una paciente con osteoporosis combinada con osteopenia.No se observó ningún efecto del alelo e4 sobre la densidad mineral ósea en la columna lumbar (prueba de Fisher, p=0,49) ,ni en el cuello femoral ( p=0,15) (
figura 2 y figura 3); se observó la misma tendencia al comparar la media de la densidad mineral ósea en los genotipos con el alelo e 4 y sin él en columna lumbar e 4+/- (e 3/ e 4 0,960±0,144 g/cm2 ); e 4+/+ (e 4/ e 4 0,873±0,00 g/cm2); e 4-/- (e 3/ e 3 0,858±0,160 g/cm2), p=0,49, y en cuello femoral e 4+/- (e 3/ e 4 0,841±0,026 g/cm2); e 4+/+ (e 4/ e 4 0,842±0,00 g/cm2); e 4-/- (e 3/ e 3 0,735±0,013 g/ cm2), p=0,14. Sin embargo, al aplicar la prueba t de Student para diferencias de medias de densidad mineral ósea en cuello femoral en los genotipos con el alelo e4 y sin él, se observó una diferencia significativa, t= 4,17, p=0,05.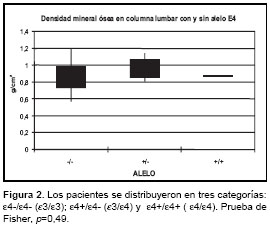
Discusión
En este estudio preliminar se confirma una frecuencia del alelo
e 4 similar a lo reportado en otros estudios realizados con población caucásica y japonesa con osteoporosis (2-5,15); la alta frecuencia del alelo e 4 en el 15,6%, comparada con el 11,6% de otros trabajos realizados con población colombiana normal (16,17) y la diferencia significativa ( p=0,05) en el análisis de las diferencias de medias en cuello femoral entre genotipos con el alelo e 4, sugiere la necesidad de otros estudios a gran escala para determinar las implicaciones de la apolipoproteína E en la salud del hueso y el riesgo de fractura. Algunos estudios revelan que las personas homocigotas para el alelo e 4 presentan niveles altos de osteocalcina en suero (4,18); en nuestro estudio se observó un caso con doble dosis para el alelo e 4 en osteoporosis combinada con osteopenia; sería importante esclarecer si el genotipo e4/ e 4 tiene asociación con la presencia de una alta reabsorción ósea o si no la tiene.Aunque no se observó ningún efecto del alelo e4 en el consumo de queso y lácteos como fuente de calcio y los hábitos de consumo de bebidas alcohólicas y cigarrillo, sería importante esclarecer el efecto de estas variables y la relación dosis efecto del genotipo APO-E en la osteoporosis aumentando el tamaño de la muestra; algunos estudios realizados con modificación de la ingestión de calcio en la dieta para ver el efecto de algunos genes sobre el metabolismo mineral, apoyan la posibilidad de que factores como el tamaño y los criterios de selección de la muestra, el estilo de vida o los factores genéticos incidan sobre los resultados de la asociación de los polimorfismos con relación a la densidad mineral ósea y fractura (19-21).
Los resultados de este estudio son el primer paso en la búsqueda de la susceptibilidad genética en la osteoporosis en la población colombiana.
Agradecimientos
Al Programa Nacional de Ciencia y Tecnología de Colciencias por su patrocinio en la realización de este trabajo, código 2104-04-11816.
A Hernán Yupanqui, Antonio Iglesias, Albenia Lurán y Aura Benavides por la oportunidad y ayuda que nos brindaron.
A Mauricio J. Vera , Franklin Prieto y Diana Giraldo por su ayuda cordial y oportuna en la realización de los análisis de resultados.
Correspondencia:
]]> Elsa Villarreal, Grupo de Nutrición, Instituto Nacional de Salud, Avenida calle 26 No. 51-60, Bogotá, D.C., ColombiaRecibido: 15/09/03; aceptado: 18/02/04
Referencias
1. Ralston SH. Genetic control of susceptibility to Osteoporosis J Clin Endocrinol 2002;87:2460-6. [ Links ]
2. Stewart TL, Ralston SH. Role of genetic factors in the pathogenesis of osteoporosis. J Endocrinol 2000;166: 235-45. [ Links ]
3. Ferrari SL, Garnero P, Emond S, Montgomery H, Humphries SE, Greenspan SL. A functional polymorphic variant in the interleukin-6-gene promoter associated with low bone resorption in portmenopausal women. Arthritis Rheum 2002;44:196-201. [ Links ]
4. Shiraki M, Shiraki Y, Aoki C, Hosoi T, Inoue S, Kaneki M. Association of bone mineral density with apolipoprotein E phenotype. J Bone Miner Res 1997; 12:1438-45. [ Links ]
5. Cauley JA, Zmuda JM, Jaffe K, Kuller LH, Ferrel RE, Wisniewski SR, Cummings SR. Apolipoprotein E polymorphism: a new genetic marker of hip fracture risk. Bone Miner Res 1999;14:1175-81. [ Links ]
6. Sadowski JA, Hood SJ, Dallal GE, Garry PJ. Phylloquinone in plasma from elderly and young adults:factors influencing its concentration. Am J Clin Nutr 1989;50:100-8. [ Links ]
7. Beavan SR, Prentice A, Stirling DM. Apolipoprotein E (APO-E) genotype and osteocalcin carboxylation postmenopause. J Bone Miner Res 1998;13:523. [ Links ]
8. Urayama S. Effect of vitamin K2 on osteoblast apoptosis: vitamin K2 inhibits apoptotic cell death of human osteoblasts induced by Fas, proteasome inhibitor, etoposide and staurosporine. J Lab Clin Med 2000;136: 181-93. [ Links ]
9. Sakami H. Apoptosis inducing activity of vitamin C and vitamin K. Cell Mol Biol 2000;46:129-43. [ Links ]
10. Carmona F. Osteoporosis en Santa Fe de Bogotá. Bogotá: Instituto Nacional de Salud; 1999. [ Links ]
11. World Health Organization. Assesment of fracture risk and its application to screening for post-menopausal osteoporosis. World technical report 845. Geneva: WHO; 1994. [ Links ]
12. Dykes D, Fondell J, Watkins P, Polesky H. A simple salting out procedure for extracting DNA from human nucleated cell. Nucleic Acids 1988;3:121. [ Links ]
13. Crock R. Single day apolipoprotein E genotyping. J Neurosci Methods 1994;2:125-7. [ Links ]
14. Wenham PR. Apolipoprotein E genotyping by one-stage PCR. Lancet 1991;337:1158-9. [ Links ]
15. Salamone LM, Dauley JA, Zmuda J, Pasagian- Macaulay A, Kuller LH. Apolipoprotein E gene polymorphism and bone loss: estrogen the influence of apolipoprotein E on bone loss. J Bone Miner Res 2000; 2:308-14. [ Links ]
16. Jaramillo-Correa JP, Keyeux G, Ruiz-García M, Rodas C, Bernal J. Population genetic analysis of the genes APO-E,APO-B (3¨VNTR) and ACE in some black and amerindian commnunities from Colombia. Hum Hered 2001;52:14-33. [ Links ]
17. Jacquier M, Arango D, Villarreal E, Torres O, Cruts M, Montañes P,Cano C, Rodriguez MN, Van Broeckhoven C. APOE epsilon 4 and Alzheimer´s disease: positive association in a Colombia clinical series and review of the Latin American studies. Arq Neuropsiquiatr 2001;59:11-7. [ Links ]
18. Kobayashi S, Inoue S, Hosoi T, Ouchi Y, Shiraki M, Orimo H. Association of bone mineral density with polymorphism of the estrogen receptor gene.J Bone Miner Res 1996;11:306-11. [ Links ]
19. Kiel DP, Myers RH, Cupples LA, Kong XF, Zhu XHl. The Bsm I vita min D receptor restriction fragment length polymorphism (bb) influences the effect of calcium intake on bone mineral density. J Bone Miner Res 1997;12:1049-57. [ Links ]
20. Salamone LM, Glyn NW, Black DM, Ferrel RE, Palermo L. Determinants of premenopausal bone mineral density: the interplay of genetic and life style factors. J Bone Miner Res 1996;11:1557-65. [ Links ]
21. Cooper GS, Umbach DM. Are vitamin D receptor polymorphism associated with bone mineral density: a meta-analysis. J Bone Miner Res 1996;11:1841-9. [ Links ] ]]>