INVESTIGACIÓN ORIGINAL
DOI 10.17533/udea.iatreia.v28n4a04
One year follow-up of the cardio-metabolic profile evolution in renal transplant patients treated with alemtuzumab, cyclosporine, and steroids in a reference hospital in Colombia
Seguimiento por un año de la evolución del perfil cardiometabólico en pacientes trasplantados renales tratados con alemtuzumab, ciclosporina y esteroides en un hospital de referencia en Colombia
Seguimento por um ano da evolução do perfil cardiometabólico em pacientes transplantados renais tratados com alemtuzumabe, ciclosporina e esteroides num hospital de referência na Colômbia
]]>
John Fredy Nieto-Ríos1; Narly Viviana Gómez-Rueda2; Lina María Serna-Higuita1; Catalina Ocampo-Kohn1; Arbey Aristizábal-Alzate1; Harry Abadía-Guzmán1; Carlos Enrique Yepes-Delgado3; Gustavo Zuluaga-Valencia1
1 Group of Nephrology and Renal Transplant, Hospital Pablo Tobón Uribe, Medellín, Colombia. lm.serna@hotmail.com; johnfredynieto@gmail.com
2 Graduate student in Internal Medicine, Pontifical Bolivarian University, 2014, Medellín, Colombia.
3 Clinical Epidemiologist, HPTU Research Unit. Tenured Professor at the Faculty of Medicine, University of Antioquia, Medellín, Colombia.
Recibido: julio 11 de 2014 ]]>
Aceptado: marzo 16 de 2015
SUMMARY
Introduction: Cardiovascular events occur 50 times more often in kidney transplant patients than in the general population and are the leading cause of death. The aim of the study was to evaluate the behavior of cardio-metabolic profile and determine the incidence of major cardiovascular events in the first year after transplantation.
Methods: This prospective study evaluated the behavior of cardio-metabolic profile in adult patients that were transplanted during 2011.
Results: The median age was 44.3 ± 12.05 years, 68.7 % were men and 95.5 %, hypertensive. Alemtuzumab-cyclosporine and steroids were used in 89.6 %, delaying the introduction of the antimetabolite. In the first year after transplantation there were three cases of diabetes mellitus, three major cardiovascular events, and 12 cases of acute rejection. Albumin, hemoglobin, weight, body mass index (BMI), calcium and HbA1C increased (p<0.05), whereas paratohormone, phosphorus, creatinine and uric acid decreased (p<0.05). Glomerular filtration rate (GFR) was higher in patients without rejection (p=0.001).
Conclusion: This immunosuppressive protocol with alemtuzumab, cyclosporine and steroids, and the delayed introduction of the antimetabolite improved bone mineral metabolism, uric acid, albumin and hemoglobin, but there were negative effects on HbA1c, weight and BMI. There was a low incidence of new onset diabetes mellitus and major cardiovascular events.
KEY WORDS
Cardiovascular Disease, Cardiovascular Risk Factors, Renal Transplantation
Introducción: en los pacientes trasplantados renales los eventos cardiovasculares ocurren 50 veces más que en la población general y son la principal causa de muerte. El objetivo del estudio fue evaluar el comportamiento del perfil cardio-metabólico y determinar la frecuencia de eventos cardiovasculares mayores en el primer año del trasplante.
Métodos: estudio prospectivo en el que se evaluó el perfil cardio-metabólico en 67 pacientes adultos trasplantados durante el 2011.
Resultados: la edad promedio fue 44,3±12,05 años, 68,7 % eran hombres y 95,5 %, hipertensos. En el 89,6 % se empleó alemtuzumab-esteroides y ciclosporina e introducción tardía del antimetabolito. Se presentaron 3 diabetes mellitus postrasplante, 3 eventos cardiovasculares mayores y 12 rechazos agudos. Al año, la albúmina, la hemoglobina, el índice de masa corporal, el calcio y la HbA1C aumentaron con respecto al valor previo al trasplante (p<0,05), mientras que la paratohormona, el fósforo, la creatinina y el ácido úrico disminuyeron (p<0,05). La tasa de filtración glomerular (TFG) al año fue mayor en los pacientes sin rechazo (p 0,001).
Conclusión: la terapia inmunosupresora con alemtuzumab- ciclosporina-esteroides mostró que al año del trasplante hubo mejoría significativa del metabolismo mineral óseo, el ácido úrico, la albúmina y la hemoglobina, pero empeoraron significativamente la HbA1c, el peso y el IMC, con una baja frecuencia de casos nuevos de diabetes mellitus y eventos cardiovasculares mayores.
PALABRAS CLAVE
Enfermedad Cardiovascular, Factores de Riesgo Cardiovascular, Trasplante Renal
RESUMO
Introdução: Nos pacientes transplantados renais os eventos cardiovasculares ocorrem 50 vezes mais do que na população geral e são a principal causa de morte. O objetivo do estudo foi avaliar o comportamento do perfil cardio-metabólico e determinar a frequência de eventos cardiovasculares maiores no primeiro ano do transplante.
Métodos: Estudo prospectivo onde se avaliou o perfil cardio-metabólico em 67 pacientes adultos transplantados durante o 2011.
]]> Resultados: A idade média foi 44,3±12,05 anos, 68,7 % homens e 95,5 % hipertensos. Em 89,6 % se empregou alemtuzumabe-esteroides e ciclosporina e introdução tardia do antimetabólito. Apresentaram-se 3 diabete mellitus pós-transplante, 3 eventos cardiovasculares maiores e 12 rejeições agudas. Ao ano, a albumina, hemoglobina, índice de massa corporal, cálcio e a HbA1C aumentaram com respeito ao valor prévio ao transplante (p<0,05), enquanto o paratormônio, fósforo, creatinina e ácido úrico diminuíram (p<0,05). A TFG ao ano foi maior nos pacientes sem rejeição (p 0,001).Conclusão: A terapia imunossupressora com alemtuzumabe- ciclosporina-esteroides mostrou que ao ano do transplante há melhoria significativa do metabolismo mineral ósseo, ácido úrico, albumina e hemoglobina mas piorou significativamente a HbA1c, o peso e o IMC, com uma baixa frequência de casos novos de diabetes mellitus e eventos cardiovasculares maiores.
PALAVRAS CHAVES
Doença Cardiovascular, Fatores de Risco Cardiovasculares, Transplante Renal
How to quote: Nieto-Ríos JF, Gómez-Rueda NV, Serna-Higuita LM, Ocampo-Kohn C, Aristizábal-Alzate A, Abadía-Guzmán H, et al. One year follow-up of the cardio-metabolic profile evolution in renal transplant patients treated with alemtuzumab, cyclosporine, and steroids in a reference hospital in Colombia. Iatreia. 2015 Oct-Dic;28(4):388-99. DOI 10.17533/udea.iatreia.v28n4a04.
INTRODUCTION
The main causes of death in renal transplant patients are cardiovascular events, followed by infection and neoplasms. Non-fatal cardiovascular events occur annually in 3.5 % to 5 % of renal transplant patients, which is 50 times higher than in the general population (1,2). Traditional risk factors are involved; however, these patients are exposed to steroids and immunosuppressive drugs that favor weight gain, insulin resistance, diabetes onset, or decompensation, and these drugs may even promote changes in lipid profiles, thus worsening baseline hypertension control (3).
However, the development of these risk factors varies among patients, possibly due to differences between baseline characteristics and the type of immunosuppressive drug used.
]]> Metabolic changes primarily occur in the first year, but cardiovascular events typically occur later. The aim of this study was to evaluate the evolution of the cardiometabolic profile and determine the frequency of major cardiovascular events 1 year after transplantation.
METHODOLOGY
This study assessed the cardio-metabolic profile of patients with end-stage chronic kidney disease (CKD) before and after transplantation between January 1 and December 31, 2011 at a high-complexity hospital in Medellin, Colombia.
All renal transplant patients over 18 years of age during the afore-mentioned period were included in the study. Electronic medical records of all identified cases were reviewed, and the following variables were also accounted for: demographic characteristics (age, sex, and race); etiology of CKD and the personal history of the recipient; donor characteristics (age, sex, and cause of death); cytomegalovirus (CMV) serostatus and donor-recipient HLA compatibility; transplant characteristics (cold ischemia time, warm ischemia time, monoclonal induction therapy, and immunosuppression protocol); and the presence of cardiovascular events, death, acute rejection, graft loss, recent onset diabetes mellitus after transplantation (NODAT) and CMV infection in the first year.
The following pre-transplant variables were determined at 3, 6 and 12 months after the procedure: creatinine (mg/dL), hemoglobin (g/dL), albumin (g/dL), calcium (mg/dL), parathyroid hormone (PTH, pg/dL), phosphorus (mg/dL), total cholesterol (mg/dL), HDL cholesterol (mg/dL), LDL cholesterol (mg/dL), triglyceride (mg/dL), fasting glucose (mg/dL), and glycosylated hemoglobin (HbA1c, %) levels; glomerular filtration rate (GFR, mL/min), weight (kg), and body mass index (BMI, kg/m2). The GFR was calculated using the Modification of Diet in Renal Disease Study (MDRD) equation (4). The following staging of post-transplant CKD was defined: stage 1, creatinine clearance >90 mL/ min; stage 2, between 60 and 89 mL/min; stage 3a, between 45 and 59 mL/min; stage 3b, between 30 and 44 mL/min; stage 4, between 15 and 29 mL/min; and stage 5, <15 mL/min.
The data were recorded in an MS-Excel® database designed for the study, and analyzed with SPSS® version 18.0 (SPSS Inc., Chicago, Illinois, USA).
The categorical variables were expressed as absolute and relative values. For continuous quantitative variables, normality assumptions were verified with the Kolmogorov-Smirnov test. Continuous quantitative variables with normal distributions were expressed as means ( x ̅ ) and standard deviation (SD). Discrete variables or those that did not fulfill the normality assumption were expressed as medians (Me) and interquartile ranges (IQR).
Inferential statistics were performed to compare variables before and after transplantation. Variable comparisons were also conducted one year after transplantation based on the presence of rejection and CKD staging after transplantation. McNemar’s test for paired data was performed for qualitative variables of related samples. For the quantitative variables, Student’s t-test for related samples was done if the difference fulfilled the assumption of normality, and a Wilcoxon test was performed when the assumption was not fulfilled. For independent samples, Student’s t-test was used to compare quantitative variables. A Kruskal-Wallis test was performed for comparisons according to the CKD stages. An alpha of 0.05 was used for all inferential statistical tests. No replacements were done for missing data.
This study was approved by the Research and Ethics Committee of the Pablo Tobon Uribe Hospital.
]]>RESULTS
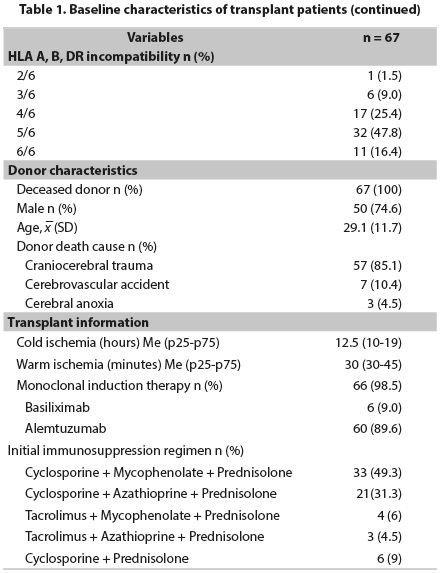
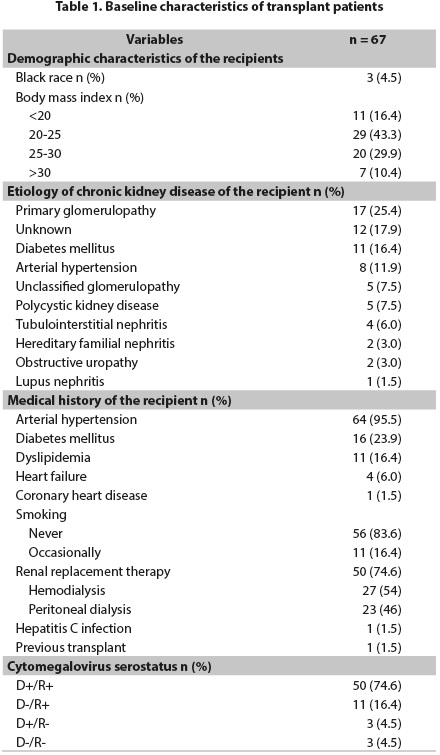
In 2011, 67 kidney transplants were performed, and 68.7 % of the patients were male. The mean age was 44.3 years (SD ± 12.05). Three patients were black. The average BMI was 24.5 kg/m2 (SD: 4.07). The main causes of CKD were primary glomerulopathies in 25.4 % followed by unknown etiologies in 17.9 %. In total, 74.6 % of the patients received renal replacement therapy before transplantation, and 54 % had hemodialysis, which was the most common type of dialysis therapy. The median time on dialysis therapy was 21 months (range: 1 month to 7 years). Regarding medical histories, arterial hypertension was present in 95.5 % of patients, and diabetes mellitus (DM) occurred in 23.9 %. One patient suffered from pre-transplant coronary artery disease, no patients were active smokers, and one patient had previously received a transplant. The donor-recipient compatibility, CMV serostatus, and other characteristics of the recipients are shown in table 1.
All transplants were performed from standard criteria deceased donors. In total, 74.6 % of donors were male with a mean age of 29.1 ± 11.7 years. The main etiology of donor brain death was craniocerebral trauma, which occurred in 85.1 % of the cases. The cold and warm ischemia times are shown in table 1.
Monoclonal antibodies were used as induction therapy in 98.5 % of the patients: six patients were treated with basiliximab, and the remaining 60 received alemtuzumab. This type of induction therapy was not used in a 60-year-old woman with a history of hepatitis C infection, in whom induction was performed with only methylprednisolone. In the immunosuppression regimen, cyclosporine was used in 80.6 % of patients as the initial calcineurin inhibitor drug, The combination regimens with antimetabolites are described in table 1.
Behavior of the metabolic profile variables of patients pre-transplant and at 3, 6, and 12 months post-transplant is shown in figure 1. The GFR was 67.98 mL/min (SD ± 19.09) 1 year after transplantation. After classifying the average GFR according to the stages of CKD (n=64 patients), 9 (14 %) patients were in stage 1, 34 (53,1 %) in stage 2, 13 (20.3 %) in stage 3a, 5 (7,8 %) in stage 3b, 2 (3,1 %) in stage 4 and 1 patient (1,6 %) in stage 5.
Events 1 year after transplantation
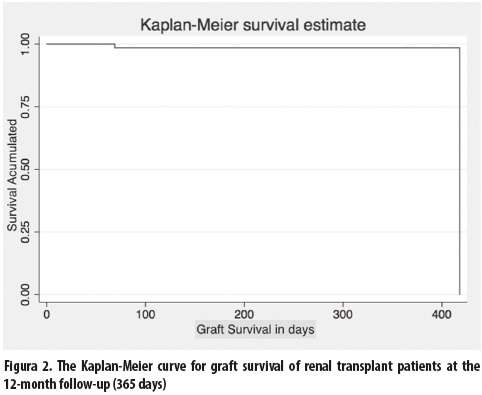
Twelve patients exhibited acute graft rejection, as confirmed by a renal biopsy. The histological report showed cellular rejection in five patients, humoral rejection in four, and mixed rejection in the remaining three. None of these patients had graft loss. Six patients required a change in immunosuppressive therapy to rapamycin pathway inhibitors: four patients due to calcineurin inhibitor toxicity, one patient due to concomitant severe infection, and the remaining one due to low-grade epithelial neoplasia. In one patient, a BK virus infection was documented. Only one patient lost the kidney graft, and this loss was secondary to the deliberate suspension of immunosuppression due to a life-threatening infection. Two patients died, one 11 days and the other 61 days after transplantation. Both of them died with a functional graft, and the cause of death in both was cardiovascular. One patient suffered an acute myocardial infarction that required endovascular therapy but did not cause death. Twelve patients suffered from CMV infections; the median time of infection was 52 days after transplantation (p25 and p75, 42 and 105 days, respectively). Survival of patients 61 days after kidney transplantiation was 97 % (figure 2).
]]>
Of the 51 patients who had no history of diabetes mellitus, three (5.8 %) developed this disease after transplantation: two of them were diagnosed with DM in the initial 3 months, and the other, at 6 months. All patients who experienced acute rejection received cyclosporine as an initial immunosuppression therapy, which was later changed to tacrolimus. No patient on the immunosuppressive therapy with tacrolimus had an initial rejection.
At 1 year, levels of albumin, hemoglobin, BMI, weight, calcium, and HbA1c were increased from the baseline values prior to the transplant and were statistically significant, whereas those of PTH, phosphorus, creatinine, and uric acid were decreased during this period (table 2). The remaining variables considered in this study, such as the LDL cholesterol, total cholesterol, triglycerides, use of antihypertensive drugs and blood glucose, were not significantly different. Renal function 1 year after transplantation was significantly different in patients who had rejection compared to those who did not have it (mean DS 51.27 ± 12.05 vs. 71.74 ± 18.42; p = 0.001). When patients were compared according to post-transplant CKD stages, levels of the different metabolic profile variables were not significantly different between the CKD stages, except for triglycerides.
DISCUSSION
The study showed that renal transplant patients had significantly improved cardio-metabolic profiles at the 1-year follow-up with respect to renal function, bone mineral metabolism, nutritional status, and anemia. However, a significant increase in the BMI and impaired carbohydrate metabolism were found, along with a low frequency of NODAT occurrence and a non-negligible frequency of major cardiovascular events. To our knowledge, few studies on this subject have been performed in Latin America. Perez A et al., reported a cardiovascular disease prevalence of 73 % in a cohort of 63 Cuban kidney transplant patients followed for 1 year; however, the study does not describe how long ago these patients were transplanted, which limits the interpretation of these data because the length of time from transplantation is directly proportional to the cardiovascular risk (5). In our study, 4.47 % (3/67) of the patients presented cardiovascular events during the first post-transplant year, which were significant. Rodelo J et al., in a Colombian series of 201 elderly kidney transplanted patients followed for 7 years, found that the main causes of death (38 %) were of cardiovascular origin; however, this was an older population with a longer follow up period, which may explain the high mortality rate (6). Roberts et al. reported an incidence of main cardiovascular events of 8.2 % (five patients with acute myocardial infarction and one with cerebrovascular disease) in a registry of the only center in Trinidad and Tobago of kidney transplanted patients (with living donors) who were followed for 5 years, but the majority of these events occurred during the first year after transplantation (three patients with acute myocardial infarction and one with cerebrovascular disease). In this paper, the weight gain, NODAT, and dyslipidemia in the first year after transplant were 21.9 %, 9.6 %, and 23 %, respectively (7).
The 1 year survival of patients was 97 %, which was similar to the results described in studies using alemtuzumab as induction therapy or in those using different inductors (8-14). The cause of death in two patients was cardiovascular, and both died with a functional graft. Both patients were diabetic, and no preventable cardiovascular cause was identified in their pre-transplant protocol. Only one patient suffered a non-fatal acute myocardial infarction, which was treated and did not affect graft function. Major cardiovascular events occurred in 4.5 % (3/67) of the patients and caused deaths in 2 patients (2.98 %). The annual risk of cardiovascular death in renal transplant patients ranged from 3.5 % to 5 %, which is 50 times higher than in the general population (1,15). This range was estimated to include a non-negligible rate of cardiovascular events due to the short follow-up time, which showed the high cardiovascular risk of these patients due to their underlying CKD and multiple comorbidities.
Censored graft survival was 98.5 %, which was higher than that reported in other series (8-10,14). Only one patient lost the graft as a result of the deliberate suspension of immunosuppression due to a life-threatening infection. The frequency of biopsy-proven rejection in this study with a regimen of alemtuzumab, cyclosporine, steroids, and the delayed introduction of antimetabolites was 17 %. All patients received the appropriate treatment according to the rejection type, and no graft losses had occurred from rejection at the one-year follow-up. Other studies of similar immunosuppression regimens report rejection rates between 10.4 % and 24 % (14,16,17). These results are similar to those described in the literature using other induction and maintenance regimens (8-13,18). This study also showed that transplant rejection significantly affected graft function (51.27 ± 12.05 vs. 71.74 ± 18.42). Several studies have reported that a lower GFR at the 1 year follow-up is a negative factor for long-term graft survival (19-21). It is important to account for the rejection rate because steroid megadoses and increased immunosuppression are used to treat rejection and could influence subsequent cardiovascular events. However, we observed no significant differences in this respect at the 1 year follow-up of our patients.
Most patients had good graft function 1 year after transplantation, as shown by an average GFR of 67.9 ± 19 mL/min, and 61 % of patients remained in stages 1 and 2 of CKD. For the different series and induction regimens available, GFR values at the 12 month follow-up have ranged from 53 to 68 mL/min (9-11,13). These results, coupled with the available evidence, demonstrate how transplantation is the best therapy for patients with CKD, not only because the disease reverts to an earlier stage but also because this treatment increases survival and improves quality of life compared to patients treated by dialysis (22-24). In the (ELITE)-Symphony study, the GFR calculated by the MDRD equation in four groups was lower than that in this study, which may be most likely explained by the younger age of our donors, and because none were extended-criteria donors (13).
Most patients quickly experienced a recovery of the biochemical properties used to assess the bone mineral profile, which was demonstrated by significant improvements in the serum PTH, calcium, and phosphorus levels within the initial 3 months, which were maintained throughout the 1-year follow-up. Similarly, hemoglobin levels significantly improved without the use of erythropoiesis-stimulating agents. Although the immunosuppression regimen was based on calcineurin inhibitors, uric acid significantly decreased without the use of hypouricemic drugs. Similar results have been previously published, and this outcome is correlated with the recovery of renal function (25-29). In patients with end-stage CKD, most cardiovascular mortality is associated with bone mineral metabolism and blood disorders, which occur up to 7.9 times more frequently than in the general population and at twice the rate observed in transplant patients. Renal transplantation is the best alternative to improve survival in these patients (22-24,30-33).
]]> Only 5.9 % of the patients in our series developed NODAT based on the standard criteria of the American Diabetes Association, which was similar to the result observed in the cyclosporine group of the (ELITE)-Symphony study and lower than the diabetes rate reported when tacrolimus was used for treatment (13,34-37). However, it should be noted that 39.2 % of the patients were classified at the 1 year follow-up as pre-diabetic according to the current guidelines. Nonetheless, we cannot interpret the significant increases observed in the HbA1c levels compared to those before transplantation due to limitations of the interpretation of HbA1c levels in patients with CKD that undergo dialysis (38-40). We believe that the above results could be explained by the drugs used and the increased BMI of patients at the 1 year followup (p < 0.001). Prior to transplantation, 38.8 % of the patients had a BMI>25. After transplantation, the percentage increased to 52.23 %, which classified the patients as overweight and obese which, according to the literature, is a determining factor for insulin resistance and impaired carbohydrate metabolism and can influence long-term cardiovascular morbidity and mortality (35,41-44).Significant increases in cholesterol and triglycerides were observed in the initial 3 months after transplantation, but with progressive improvement in subsequent months and levels similar to those observed pre-transplant at the 1 year follow-up. The initial increase was explained by the effect of immunosuppressive drugs on lipoproteins, and the subsequent improvement was explained by the increased use of oral lipid-lowering drugs, which, in this study, increased from 26.9 % prior to transplantation to 55.2 % at the 1 year follow-up. Dyslipidemia is considered a known cardiovascular risk factor, and its association with cardiovascular disease has been demonstrated in several studies with longer follow-ups (1,45-47).
Among the limitations of this study, we should note that it was performed in a single clinical center, to which patients were referred by their insurers with an indication for renal transplantation, resulting in the possibility of a selection bias for patients with better baseline statuses, better social support, and better pre-transplant health insurance coverage. A 1 year follow-up of a patient is a short period to correlate cardio-metabolic variables with clinically important cardiovascular outcomes, coupled with the inability to follow-up some patients due to the requirements imposed by insurance companies. Blood chemistry measurements were performed in different laboratories, thus making it difficult to standardize the results. The power to demonstrate differences in subgroups according to the stage of CKD was limited by the small sample size. The ability to perform clinical and paraclinical follow-ups in 90 % of patients was one of the strengths of our transplant group and the study.
In conclusion, patients with CKD have multiple cardio-metabolic abnormalities that improve with renal transplantation; however, this population continues to exhibit non-negligible multiple modifiable risk factors and major cardiovascular outcomes at the 1 year follow-up. The authors recommend the follow-up and treatment of these factors, which can influence short- and long-term cardiovascular morbidity and mortality.
CONFLICT OF INTEREST STATEMENT
The authors declare that there is no conflict of interest in this study. Its results have not been published previously.
ACKNOWLEDGEMENTS
The authors wish to thank Pablo Tobon Uribe Hospital.
]]>BIBLIOGRAPHIC REFERENCES
1. Ojo AO. Cardiovascular complications after renal transplantation and their prevention. Transplantation. 2006 Sep;82(5):603-11. [ Links ]
2. Wauters RP, Cosio FG, Suarez Fernandez ML, Kudva Y, Shah P, Torres VE. Cardiovascular consequences of new-onset hyperglycemia after kidney transplantation. Transplantation. 2012 Aug;94(4):377-82. [ Links ]
3. Cohen DJ, Vella JP. Nephrology Self-Assessment Program. Transplantation. Am Soc Nephrol. 2011 Nov;10(6):525-614. [ Links ]
4. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999 Mar;130(6):461-70. [ Links ]
]]>5. Pérez Rodriguez A, Leyva de la Torre C, Enamorado Casanova A, Pérez de Prado JC, Gutiérrez García F, Rodríguez Torres JC. Enfermedad Cardiovascular en Pacientes Con Trasplante Renal. Rev Cuba Med. 2014; 53(1): 37-49. [ Links ]
6. Rodelo JR, Nieto-Ríos JF, Serna-Higuita LM, Henao JE, García A, Reino AC, et al. Survival of renal transplantation patients older than 60 years: a single-center experience. Transplant Proc. 2013 May;45(4):1402-9. [ Links ]
7. Roberts L, Ramsaroop K, Seemungal T. Survival outcomes in renal transplantation in Trinidad and Tobago: SORTTT study. West Indian Med J. 2012 Jul;61(4):422-8. [ Links ]
8. Hanaway MJ, Woodle ES, Mulgaonkar S, Peddi VR, Kaufman DB, First MR, et al. Alemtuzumab induction in renal transplantation. N Engl J Med. 2011 May;364(20):1909-19. [ Links ]
9. Welberry Smith MP, Cherukuri A, Newstead CG, Lewington AJ, Ahmad N, Menon K, et al. Alemtuzumab induction in renal transplantation permits safe steroid avoidance with tacrolimus monotherapy: a randomized controlled trial. Transplantation. 2013 Dec;96(12):1082-8. [ Links ]
]]>10. Brennan DC, Flavin K, Lowell JA, Howard TK, Shenoy S, Burgess S, et al. A randomized, double-blinded comparison of Thymoglobulin versus Atgam for induction immunosuppressive therapy in adult renal transplant recipients. Transplantation. 1999 Apr;67(7):1011-8. Erratum in: Transplantation 1999 May;67(10):1386. [ Links ]
11. Brennan DC, Daller JA, Lake KD, Cibrik D, Del Castillo D; Thymoglobulin Induction Study Group. Rabbit antithymocyte globulin versus basiliximab in renal transplantation. N Engl J Med. 2006 Nov;355(19):1967-77. [ Links ]
12. Ciancio G, Burke GW, Gaynor JJ, Roth D, Kupin W, Rosen A, et al. A randomized trial of thymoglobulin vs. alemtuzumab (with lower dose maintenance immunosuppression) vs. daclizumab in renal transplantation at 24 months of follow-up. Clin Transplant. 2008 Mar-Apr;22(2):200-10. [ Links ]
13. Ekberg H, Tedesco-Silva H, Demirbas A, Vítko S, Nashan B, Gürkan A, et al. Reduced exposure to calcineurin inhibitors in renal transplantation. N Engl J Med. 2007 Dec;357(25):2562-75. [ Links ]
14. Farney AC, Doares W, Rogers J, Singh R, Hartmann E, Hart L, et al. A randomized trial of alemtuzumab versus antithymocyte globulin induction in renal and pancreas transplantation. Transplantation. 2009 Sep;88(6):810-9. [ Links ]
]]>15. Aakhus S, Dahl K, Widerøe TE. Cardiovascular disease in stable renal transplant patients in Norway: morbidity and mortality during a 5-yr follow-up. Clin Transplant. 2004 Oct;18(5):596-604. [ Links ]
16. Watson CJ, Bradley JA, Friend PJ, Firth J, Taylor CJ, Bradley JR, et al. Alemtuzumab (CAMPATH 1H) induction therapy in cadaveric kidney transplantation- -efficacy and safety at five years. Am J Transplant. 2005 Jun;5(6):1347-53. [ Links ]
17. Ocampo C, Aristizabal A, Nieto J, Abadia H, Angel W, Guzman C, et al. Induction therapies in kidney transplantation: the experience of Hospital Pablo Tobon Uribe, Medellín, Colombia 2005-2010. Transplant Proc. 2011 Nov;43(9):3359-63. [ Links ]
18. Clatworthy MR, Friend PJ, Calne RY, Rebello PR, Hale G, Waldmann H, et al. Alemtuzumab (CAMPATH-1H) for the treatment of acute rejection in kidney transplant recipients: long-term follow-up. Transplantation. 2009 Apr;87(7):1092-5. [ Links ]
19. Resende L, Guerra J, Santana A, Mil-Homens C, Abreu F, da Costa AG. First year renal function as a predictor of kidney allograft outcome. Transplant Proc. 2009 Apr;41(3):846-8. [ Links ]
]]>20. Fonseca I, Almeida M, Martins LS, Santos J, Dias L, Lobato L, et al. First-year renal function predicts longterm renal allograft loss. Transplant Proc. 2011 Jan- Feb;43(1):106-12. [ Links ]
21. Guerra J, Raimundo M, Teixeira C, Santana A, Cortesão A, Gomes da Costa A. Factors that may influence estimated glomerular filtration rate in patients with excellent graft function 10 years posttransplant. Transplant Proc. 2013 Apr;45(3):1060-2. [ Links ]
22. Kontodimopoulos N, Niakas D. An estimate of lifelong costs and QALYs in renal replacement therapy based on patients life expectancy. Health Policy. 2008 Apr;86(1):85-96. [ Links ]
23. Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999 Dec;341(23):1725-30. [ Links ]
24. Rebollo P, Ortega F, Baltar JM, Díaz-Corte C, Navascués RA, Naves M, et al. Health-related quality of life (HRQOL) in end stage renal disease (ESRD) patients over 65 years. Geriatr Nephrol Urol. 1998;8(2):85-94. [ Links ]
]]>25. Evenepoel P, Claes K, Kuypers D, Maes B, Bammens B, Vanrenterghem Y. Natural history of parathyroid function and calcium metabolism after kidney transplantation: a single-centre study. Nephrol Dial Transplant. 2004 May;19(5):1281-7. [ Links ]
26. Reinhardt W, Bartelworth H, Jockenhövel F, Schmidt- Gayk H, Witzke O, Wagner K, et al. Sequential changes of biochemical bone parameters after kidney transplantation. Nephrol Dial Transplant. 1998 Feb;13(2):436-42. [ Links ]
27. Jones H, Talwar M, Nogueira JM, Ugarte R, Cangro C, Rasheed H, et al. Anemia after kidney transplantation; its prevalence, risk factors, and independent association with graft and patient survival: a time-varying analysis. Transplantation. 2012 May;93(9):923-8. [ Links ]
28. Lofaro D, Greco R, Papalia T, Bonofiglio R. Increasing levels of hemoglobin improve renal transplantation outcomes. Transplant Proc. 2011 May;43(4):1036-8. [ Links ]
29. Chung BH, Kang SH, Hwang HS, Choi BS, Park CW, Kim YS, et al. Clinical significance of early-onset hyperuricemia in renal transplant recipients. Nephron Clin Pract. 2011;117(3):c276-83. [ Links ]
]]>30. Rabbat CG, Thorpe KE, Russell JD, Churchill DN. Comparison of mortality risk for dialysis patients and cadaveric first renal transplant recipients in Ontario, Canada. J Am Soc Nephrol. 2000 May;11(5):917-22. [ Links ]
31. Oniscu GC, Brown H, Forsythe JL. Impact of cadaveric renal transplantation on survival in patients listed for transplantation. J Am Soc Nephrol. 2005 Jun;16(6):1859-65. [ Links ]
32. Port FK, Wolfe RA, Mauger EA, Berling DP, Jiang K. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA. 1993 Sep;270(11):1339-43. [ Links ]
33. United States Renal Data System. Annual Data Report 2014: an overview of the Epidemiology of Kidney Disease in the United States [Internet]. Bethesda: NIH; 2014 [consultado 2014 Feb 23]. Disponible en: http://www.usrds.org/adr.aspx [ Links ]
34. American Diabetes Association. Standards of medical care in diabetes--2014. Diabetes Care. 2014 Jan;37 Suppl 1:S14-80. [ Links ]
35. Heisel O, Heisel R, Balshaw R, Keown P. New onset diabetes mellitus in patients receiving calcineurin inhibitors: a systematic review and meta-analysis. Am J Transplant. 2004 Apr;4(4):583-95. [ Links ]
36. Vincenti F, Friman S, Scheuermann E, Rostaing L, Jenssen T, Campistol JM, et al. Results of an international, randomized trial comparing glucose metabolism disorders and outcome with cyclosporine versus tacrolimus. Am J Transplant. 2007 Jun;7(6):1506-14. Erratum in: Am J Transplant. 2008 Jan;8(1):1. Am J Transplant. 2008 Apr;8(4):908. [ Links ]
37. Burroughs TE, Lentine KL, Takemoto SK, Swindle J, Machnicki G, Hardinger K, et al. Influence of early posttransplantation prednisone and calcineurin inhibitor dosages on the incidence of new-onset diabetes. Clin J Am Soc Nephrol. 2007 May;2(3):517-23. [ Links ]
38. Inaba M, Okuno S, Kumeda Y, Yamada S, Imanishi Y, Tabata T, et al. Glycated albumin is a better glycemic indicator than glycated hemoglobin values in hemodialysis patients with diabetes: effect of anemia and erythropoietin injection. J Am Soc Nephrol. 2007 Mar;18(3):896-903. [ Links ]
39. Ng JM, Cooke M, Bhandari S, Atkin SL, Kilpatrick ES. The effect of iron and erythropoietin treatment on the A1C of patients with diabetes and chronic kidney disease. Diabetes Care. 2010 Nov;33(11):2310-3. [ Links ]
40. Shabir S, Jham S, Harper L, Ball S, Borrows R, Sharif A. Validity of glycated haemoglobin to diagnose new onset diabetes after transplantation. Transpl Int. 2013 Mar;26(3):315-21. [ Links ]
41. Kasiske BL, Snyder JJ, Gilbertson D, Matas AJ. Diabetes mellitus after kidney transplantation in the United States. Am J Transplant. 2003 Feb;3(2):178-85. [ Links ]
42. Bayer ND, Cochetti PT, Anil Kumar MS, Teal V, Huan Y, Doria C, et al. Association of metabolic syndrome with development of new-onset diabetes after transplantation. Transplantation. 2010 Oct;90(8):861-6. [ Links ]
43. Cosio FG, Kudva Y, van der Velde M, Larson TS, Textor SC, Griffin MD, et al. New onset hyperglycemia and diabetes are associated with increased cardiovascular risk after kidney transplantation. Kidney Int. 2005 Jun;67(6):2415-21. [ Links ]
44. Santos L, Rodrigo E, Piñera C, Quintella E, Ruiz JC, Fernández-Fresnedo G, et al. New-onset diabetes after transplantation: drug-related risk factors. Transplant Proc. 2012 Nov;44(9):2585-7. [ Links ]
45. Jardine AG, Gaston RS, Fellstrom BC, Holdaas H. Prevention of cardiovascular disease in adult recipients of kidney transplants. Lancet. 2011 Oct;378(9800):1419-27. [ Links ]
46. Holdaas H, Fellström B, Holme I, Nyberg G, Fauchald P, Jardine A, et al. Effects of fluvastatin on cardiac events in renal transplant patients: ALERT (Assessment of Lescol in Renal Transplantation) study design and baseline data. J Cardiovasc Risk. 2001 Apr;8(2):63-71. [ Links ]
47. Holdaas H, Fellström B, Jardine AG, Nyberg G, Grönhagen-Riska C, Madsen S, et al. Beneficial effect of early initiation of lipid-lowering therapy following renal transplantation. Nephrol Dial Transplant. 2005 May;20(5):974-80. [ Links ]
]]>