PRESENTACIÓN DE CASO
DOI 10.17533/udea.iatreia.v29n1a07
Heterotopic mesenteric ossification in a child: Case report
Osificación mesentérica heterotópica en un niño: informe del caso
Ossificação mesentérica heterotópica num menino: relatório do caso
]]>
Natalia Herrera-Toro1; Francisco Javier Mejía-Sarasti2
1 Cirujana general y pediátrica. Profesora, Facultad de Medicina, Universidad de Antioquia, Medellín, Colombia. Cirujana pediátrica, Hospital Pablo Tobón Uribe, Medellín, Colombia. nataherrerat@gmail.com
2 Cirujano pediátrico, Hospital Pablo Tobón Uribe, Medellín, Colombia.
Recibido: abril 08 de 2015
Aceptado: abril 15 de 2015
SUMMARY
The term heterotopic ossification refers to bone formation in normally non-ossifying tissue. It represents a benign, localized, self-limiting and well-circumscribed lesion, and the phenomenon is rather unusual in the immediate vicinity of bones. Likewise, it is very rare in soft tissues such as the gastrointestinal tract, where it is also known as heterotopic mesenteric ossification (HMO). Intra-abdominal heterotopic ossification (IHO) is also known as intra-abdominal myositis ossificans, mesenteritis ossificans, heterotopic mesenteric ossification, and heterotopic ossification of the intestinal mesentery. It is extremely rare and only approximately 30 cases have been reported in the literature since it was first described in 1983. This paper presents the case of a male 14 year-old patient diagnosed with mesenteric ossification who was treated by the pediatric surgeons. Additionally, the authors present a review of the medical literature regarding this condition.
KEY WORDS
Digestive System Fistula, Intestinal Obstruction, Mesentery, Ossification Heterotopic, Osteogenesis
RESUMEN
El término osificación heterotópica se refiere a la neoformación de tejido óseo en sitios donde normalmente el tejido no se osifica. Es una condición benigna, localizada, bien definida y autolimitada; ocurre con mayor frecuencia en la vecindad inmediata de los huesos. Es muy raro que se presente en los tejidos blandos del tracto gastrointestinal, donde es conocida como osificación heterotópica del mesenterio (OHM). La osificación heterotópica intraabdominal (OHI) es además conocida como miositis osificante, mesenteritis osificante, osificación heterotópica del mesenterio y osificación heterotópica del mesenterio intestinal. Es una condición extremadamente rara, con solo 30 casos aproximadamente reportados en la literatura desde su primera descripción en 1983. Este artículo presenta el caso de un niño de 14 años con diagnóstico de mesenteritis osificante que fue tratado por un grupo de cirujanos pediátricos. Además, se presenta una revisión de la literatura médica sobre esta extraña condición.
PALABRAS CLAVE
Fístula del Sistema Digestivo, Mesenterio, Obstrucción Intestinal, Osificación Heterotópica, Osteogénesis
O termo ossificação heterotópica se refere à neoformação de tecido ósseo em lugares onde normalmente o tecido não se ossifica. É uma condição benigna, localizada, bem definida e autolimitada; ocorre com maior frequência na vizinhança imediata dos ossos. É muito raro que se apresente nos tecidos macios do trato gastrointestinal, onde é conhecida como ossificação heterotópica do mesentério (OHM). A ossificação heterotópica intra-abdominal (OHI) é ademais conhecida como miosite ossificante, mesenterites ossificante, ossificação heterotópica do mesentério e ossificação heterotópica do mesentério intestinal. É uma condição extremamente rara, com só 30 casos aproximadamente reportados na literatura desde sua primeira descrição em 1983. Este artigo apresenta o caso de um menino de 14 anos com diagnóstico de mesenterites ossificante que foi tratado por um grupo de cirurgiões pediátricos. Ademais, apresenta-se uma revisão da literatura médica sobre esta estranha condição.
PALAVRAS CHAVE
Fístula do sistema digestivo, Mesentério, Obstrução intestinal, Ossificação Heterotópica, Osteogêneses
Cómo citar: Herrera-Toro N, Mejía-Sarasti FJ. Heterotopic mesenteric ossification in a child: Case report. Iatreia. 2016 Jan-Mar;29(1):75-80. DOI 10.17533/udea.iatreia.v29n1a07.
INTRODUCTION
The presence of heterotopic bones in the gastrointestinal tract is very rare. Mesenteritis ossificans, also known as heterotopic mesenteric ossification (HMO), refers to a reactive bone formation in the adipose tissue of the mesentery which is frequently related to repetitive abdominal surgery, tumors, intra-abdominal infections, or trauma. However, the pathological mechanisms are yet to be determined. This pathology may often be accompanied by intestinal obstructions or recurrent enterocutaneous fistulas. This paper presents the case of a patient treated by the pediatric surgery group of a high-complexity level hospital.
]]> CASE REPORT
The patient was a 14-year-old male with a history of high anorectal malformation and rectourethral fistula, first requiring a neonatal colostomy and then posterior sagittal anorectoplasty. Colostomy closure was performed after one year. The patient also had a history of tethered spinal cord syndrome with surgical decompression at age two. Secondary to these pathologies were neurogenic colon and bladder, which were treated through augmentation ileocystoplasty and a Mitrofanoff continent urinary diversion of the bladder. Similarly, a Malone continent ostomy of the cecal appendix was carried out in order to perform antegrade enemas for controlling the neurogenic colon.
The patient consulted a doctor due to symptoms of the Malone ostomy obstruction associated with soft tissue abscess. Treatment consisted of draining the collection and performing the Malone procedure again. In the postoperative period cecal ischemia was observed together with intestinal leakage and fecal peritonitis. The patient required surgical interventions with ileostomy, open abdomen management to wash the peritoneal cavity, implantation of a vacuumassisted wall closure system with negative pressure and, subsequently, abdominal wall closure using polypropylene mesh. He was discharged and showed adequate progress.
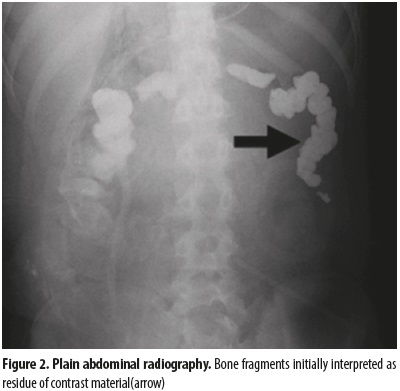
Fifteen days later, the patient was admitted with symptoms of intestinal obstruction and stool output through the surgical wound. An entero-cutaneous fistula was diagnosed and treatment for both conditions was initiated. An upper gastrointestinal tract X-ray test was done which confirmed the presence of the fistula and showed that it was located in the proximal jejunum, which was inconsistent with the clinical findings. Additionally, an abdominal CT was performed which showed changes due to mesenteritis (figure 1).
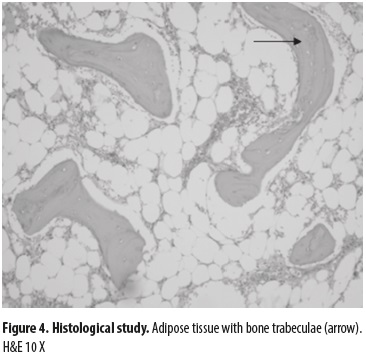
Given that the patient did not improve as a result of the medical treatment, and that new fistulas appeared, a barium enema test was requested. The simple X-ray results of this test described the persistence of the contrast material (figure 2). Consequently, surgery was conducted which showed that the particles that had been described were actually bone residues in the mesentery.
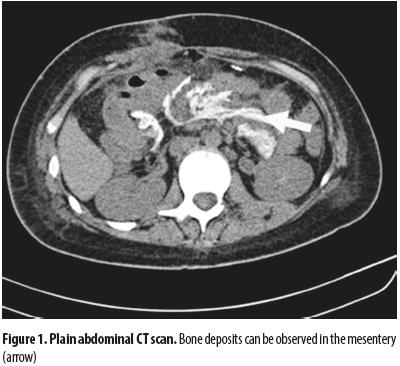
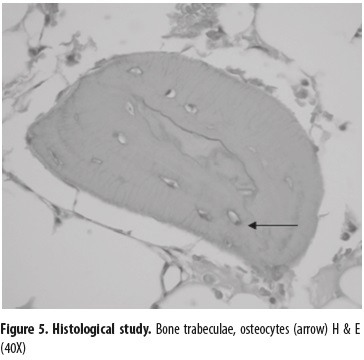
During surgery the abdomen was found to be blocked by a severe adhesion syndrome, five intestinal fistulas associated with the presence of multiple bone spicules, and by the ossification of almost all of the mesentery. Adhesiolysis was performed and the entero-cutaneous fistulas were closed. The bone lesions were partially removed (figure 3) and samples were sent to pathology, which confirmed the diagnosis of mesenteritis ossificans (figures 4 and 5).
]]>
DISCUSSION
Heterotopic mesenteric ossification (HMO) is a rare bone-producing alteration that takes place in the mesentery. It was first proposed by Wilson; however there were previous descriptions of a pseudo-malignant bone tumor of the connective tissue or intraabdominal myositis ossificans (1).
The etiology and pathogenesis of this condition are unknown. It has been found associated with trauma, intra-abdominal surgeries such as laparotomies in predisposed patients, intra-abdominal infections, venous stasis, ischemia, edema, inflammation (2) or in the presence of mucinous epithelial tumors (3,4). It has also been reported to be associated with benign polyps, carcinomas, colon and stomach carcinoid tumors and mucoceles of the appendix (5). Most patients had previously undergone abdominal surgery. The lesions had a tendency to grow and developed within weeks or even days after the surgical procedure (6).
The age of onset for HMO falls within a wide range. Reports of its appearance range from 22 to 80 years old (7); however, most of the patients described in the literature have been middle-aged individuals, mostly males, between the ages of 40 and 80. There are no reports of patients in the pediatric age. Symptoms are usually based on recurrent intestinal obstruction and enterocutaneous fistulas (8), and the precise pathological mechanisms for heterotopic ossification remain unsolved. It has been suggested that the osteoblastic metaplasia is a response to multipotent mesenchymal cell trauma and an inflammatory reaction with the transformation of fibroblasts and adipose tissue into bone cells. No malignant potential has been found, but morbidity is attributed to it because of its capacity to block the intestines. The presence of reactive sites resembling nodular fascitis, osteoid thickening, and the absence of nuclear atypia, necrosis and atypical mitotic figures make it possible to differentiate this condition from osteosarcoma and other malignant lesions, such as lipomiosarcoma (9,10).
There are several theories explaining heterotopic ossification mechanisms: 1) bone formation occurs because of the implantation of small particles containing osteogenic cells from the perichondrium or periosteum that are planted during a laparotomy or trauma; 2) bone formation is caused by differentiated stem cells in the mesoblast, as well as in the osteoblasts or chondroblasts, which result from local lesions, inflammatory processes, or infectious stimuli.
Preoperative diagnosis is sometimes difficult; abdominal CT scans can provide evidence of the pathology, yet radiological differentiation between mesenteritis ossificans, dystrophic calcification, bone neoplasms, and intestinal leakage of contrast material may be difficult (11).
Heterotopic mesenteric ossification is considered to have good prognosis; however, it becomes a challenge once it appears since it tends to return. In some cases, the condition manifests itself through intestinal obstruction and requires intestinal resection. Despite this, since the condition has been associated with surgery, repeated surgical procedures should be avoided (4,12). In this case the condition was very aggressive and was accompanied by intestinal obstruction and multiple hard to treat entero-cutaneous fistulas. The patient required complete resection of the affected mesentery, and of the small intestine from the duodenum to the ileum. Treatment involved total parenteral nutrition, and the patient was included in the waiting list for intestinal transplant.
]]> BIBLIOGRAPHIC REFERENCES
1. Ibáñez Alonso S, Peña Sarnago JM, Insausti Jaca N, Atilano Santos L. Mesenteritis osificante. Radiología. 2007;49:51-2. [ Links ] DOI 10.1016/S0033-8338(07)73717-7.
2. Wilson JD, Montague CJ, Salcuni P, Bordi C, Rosai J. Heterotopic mesenteric ossification ('intraabdominal myositis ossificans'): report of five cases. Am J Surg Pathol. 1999 Dec;23(12):1464-70. [ Links ]
3. Bovo G, Romano F, Perego E, Franciosi C, Buffa R, Uggeri F. Heterotopic mesenteric ossification (''intraabdominal myositis ossificans''): a case report. Int J Surg Pathol. 2004 Oct;12(4):407-9. [ Links ]
4. Zamolyi RQ, Souza P, Nascimento AG, Unni KK. Intraabdominal myositis ossificans: a report of 9 new cases. Int J Surg Pathol. 2006 Jan;14(1):37-41. [ Links ]
5. Yasuma T, Hashimoto K, Miyazawa R, Hiyama Y. Bone formation and calcification in gastric cancer--case report and review of literature. Acta Pathol Jpn. 1973 Feb;23(1):155-72. [ Links ]
6. Hansen O, Sim F, Marton PF, Grüner OP. Heterotopic ossification of the intestinal mesentery. Report of a case following intraabdominal surgery. Pathol Res Pract. 1983 Mar;176(2-4):125-30. [ Links ]
7. Fletcher CDM, Unni KK, Mertens F, editors. Pathology and genetics of tumours of soft tissue and bone. Lyon: IARC; 2000. [ Links ]
8. Yushuva A, Nagda P, Suzuki K, Llaguna OH, Avgerinos D, Goodman E. Heterotopic mesenteric ossification following gastric bypass surgery: case series and review of literature. Obes Surg. 2010 Sep;20(9):1312-5. [ Links ] DOI 10.1007/s11695-009-0072-8.
9. Patel RM, Weiss SW, Folpe AL. Heterotopic mesenteric ossification: a distinctive pseudosarcoma commonly associated with intestinal obstruction. Am J Surg Pathol. 2006 Jan;30(1):119-22. [ Links ]
10. Nascimento AG, Kurtin PJ, Guillou L, Fletcher CD. Dedifferentiated liposarcoma: a report of nine cases with a peculiar neurallike whorling pattern associated with metaplastic bone formation. Am J Surg Pathol. 1998 Aug;22(8):945-55. [ Links ]
11. Tonino BA, van der Meulen HG, Kuijpers KC, Mallens WM, van Gils AP. Heterotropic mesenteric ossification: a case report (2004:10b). Eur Radiol. 2005 Jan;15(1):195-7. [ Links ]
12. Yannopoulos K, Katz S, Flesher L, Geller A, Berroya R. Mesenteritis ossificans. Am J Gastroenterol. 1992 Feb;87(2):230-3. [ Links ]
]]>