










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.4 Bogotá Oct./Dec. 2011
Bloating and abdominal distention: Just gas? A look in the direction of physiology
David B. Páramo Hernández, MD. (1)
(1) Professor of Clinical Gastroenterology at Santa Clara Hospital, Clínica Universitaria Universidad de La Sabana, Bogotá Colombia
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 02-11-11 Accepted: 22-11-11
Abstract
Many patients with functional digestive disorders such as irritable bowel syndrome (IBS) complain of bloating, abdominal distention and similar symptoms. Until recently these symptoms have been poorly understood, however new research allows us to clarify some aspects of their pathophysiology. This review discusses some aspects of these symptoms which are related to intestinal gas and its transit, visceral hypersensitivity, viscerosomatic response and to the intestinal microbiota.
Key words
Distention, bloating, irritable bowel syndrome (IBS), pathophysiology.
INTRODUCTION
Bloating and abdominal distention
Among the various types of functional digestive disorders common discomforts such as bloating and abdominal distention which are apparently safe can produce significant alterations to a patients quality of life especially when they are within the framework of conditions such as irritable bowel syndrome (1). The Spanish lexicon includes distensión abdominal (abdominal distention), but borrows bloating from English without clearly differentiating the meanings of these terms as in English where bloating means the subjective sensation of abdominal distention and "abdominal distention" means the visible symptom or objective assessment found in a clinical examination. The latest edition of the Rome III Diagnostic Criteria for Functional Gastrointestinal Disorders (FGDs) from the Rome Foundation (2, 3) includes "Functional Bloating" in C2 of the section on Functional Intestinal Disorders. It defines "Functional Bloating" as a condition not associated with other intestinal or gastroduodenal disorders since its criteria are based on symptoms. It goes on to say that it is a feeling of abdominal distention which may or may not be associated with measurable distention. This allows us to infer that the symptom and the sign may be present under the same denomination.
Now, to perform the official Spanish translation supported by the Translations Committee of the Rome Foundation, the Mexican Gastroenterology magazine translates the term "C2: Functional Bloating" as "C2 Inflamación / Distensión Funcional." To the diagnostic criteria they add another word "Hinchazón" as follows: "Sensación recurrente de inflamación/ hinchazón o distensión visible cuando menos tres días al mes en los últimos tres meses."4 The result is, at the least, a little confusing because the words inflamación and hinchazón mean "inflammation and swelling" which are organic rather than functional.
Abdominal inductance plethysmography and abdominal computed axial tomography have demonstrated convincingly that abdominal distention does occur in IBS patients reaching 4.72 additional inches of abdominal circumference in some patients (5). Even though the bloating sensation and visible abdominal distention may occur together, they do not always occur together, for while many IBS patients complain of bloating only about half objectively demonstrate abdominal distention (5, 6).
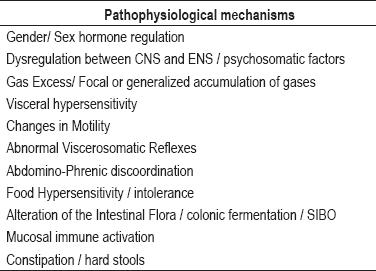
Given these difficulties, the purpose of this review is to check different perspectives addressing the problem from the pathophysiological point of view. Table 1 presents these perspectives without attempting to resolve differences in linguistic terms or in clinical characteristics.
Table 1. Bloating y abdominal distention.
EPIDEMIOLOGY
Functional Bloating is a frequently occurring functional intestinal disorder. It is typically exacerbated by meals, fluctuates in intensity, worsens at the end of the day and may increase in the middle of the night. Population research estimates prevalence from 16% to 30 % (7), but over 90% of IBS patients suffer from abdominal distention, and twice as many women as men suffer from this condition (8). While it may be present in both IBS subtypes, its prevalence varies from 40% in diarrhea-predominant IBS to 75% in constipation-predominant IBS (9). While healthy women report changes in their bowel habits during menstruation, 40% to 75% of IBS patients report that abdominal distention is exacerbated prior to menstruation suggesting the possibility of hormonal influence in the symptoms variability (8).
PATHOGENESIS
1. Psychosocial Factors
It is clear that abdominal distention´s symptoms are FGDs with mechanisms similar in pathophysiology including key components in its genesis such as psychosocial factors. In recent years advances in comprehension of FGDs pathophysiology have included interesting developments ranging from very significant in childhood psychosocial factors such as trauma and abuse to alterations in neural functioning in the anterior cingulate cortex (10, 11).
Nevertheless, the relation of psychosocial factors to bloating and abdominal distension remains controversial because many patients relate symptoms with stress (8) while symptomatic patients have no clinical anxiety or depression (12). What is most likely involved in these symptoms is dysregulation of management of, and response to, afferent information between the central nervous system and the enteric nervous system secondary to psychosocial factors (11).
2. The role of gas
Excess gas
Many patients with IBS who complain of functional bloating are convinced that this is due to increased abdominal gas content. This could easily occur through fermentation of undigested carbohydrates by colonic bacteria or result from increased swallowing of air (13). Nevertheless, gas washing techniques and CAT scans combined with modern imaging analysis software have shown that this is not the main problem in most patients, but rather defects in distribution and transit of gas are more often the source of problems (14).
Gas transit
In a study of gas infusion into the jejunum in healthy volunteers and IBS patients, 18 of 20 IBS patients retained gas and developed distention or abdominal symptoms, but these symptoms did not occur in 16 out of 20 volunteers (15). These changes can be increased by adding an enteral lipid infusion which might provide an explanation for postprandial bloating (18). Additional experience evaluating oral-cecal and colonic transit with the use of abdominal inductance plethysmography could establish whether oral-cecal and colonic transit is directly related to abdominal distention among IBS patients, and whether they are inversely rated with stool consistency (17). Similar findings from research using scintigraphic techniques with radioactive xenon were recently published. Patients with constipation predominant IBS showed impaired clearance of a load of gas in the right colon and had increased sensations of bloating plus increased abdominal distension as measured by abdominal circumference (18).
3. Dysfunctional visceral sensitivity
It is well established that a great proportion of IBS patients have visceral hypersensitivity which might contribute to bloating (7), especially since normal stimulus or small variations of the gas content inside the bowel can be perceived as bloating by patients with these functional disorders (19, 20).
Visceral hypersensitivity can be measured by neuroendocrine factors, increased intestinal permeability, alteration in gastrointestinal afferent impulses and by their processing in the central nervous system (19). It has also been found that autonomous nervous system modulates visceral hypersensitivity and it is known that increased sympathetic tone increases the levels of perception of intestinal stimuli (21). Since some IBS patients have increased sympathetic activity, this mechanism could play a key role in bloating (22). It is also recognized that IBS patients have increased mental attention to intestinal stimuli hence those presenting bloating pay more attention to their abdomen which is a kind of hyper-vigilance of their abdomen and all that comes from the bowels (22, 23).
Clinical experience shows that there is a relation between bloating without objective distention and the presence of visceral hypersensitivity. On the other hand when the abdominal circumference is enlarged during the course of the day it is more often associated with hyposensitivity and constipation-predominant IBS (24, 25).
4. Somatic dysfunction and abdomino-phrenic dyssynergia
This is one of the most recent pathophysiological developments of interest uncovered by groups investigating bloating. Mechanical mechanisms which have been proposed include diaphragmatic depression, hyperlordosis, weakness of the abdominal musculature and protrusion of the abdomen. Voluntary control of the abdominal musculature has also been suggested but its verification has been contested (26). It can be assumed that there is some type of innate reflex of the muscles of the anterior wall that allow adjustment of the bowel to ingestion of meals, to the pregnant uterus, or to change in posture as in standing or sitting. It is possible that this reflex is altered or exaggerated in patients with bloating (7, 29). The Barcelona Group used electromyography and sophisticated analysis of CAT scans in a study of volunteers and patients with IBS and/or bloating to show that abdominal adjustment to the load of volume is an active process that involves responses of the abdominal and diaphragm muscles (27). Patients with IBS and/or bloating have altered visceral-somatic reflexes with abdominal wall dystonia and failure of tonic contractions of the muscles combined with a paradoxical relaxation of the internal oblique muscles in response to a load of gas (28). Another study by the same group (30) compared patients whose main complaint was bloating with patients with severe intestinal dysmotility. CAT scans were performed on all patients in both groups in basal conditions and during the episodes of severe bloating. There were no differences at basal levels, but during bloating episodes patients with dysmotility showed a real increase of the total abdominal volume with a cephalic displacement of the diaphragm, whereas patients with functional disorders showed only small increases of intraabdominal volume. Distention was related to lowering of the diaphragm resulting from ventral-caudal distribution of content (39). These findings are of great value because they demonstrate that abnormal visceral-somatic reflexes generate abdominal distention (31). Another element of great value in this research is the addition of another diagnostic criterion for differentiating between functional and organic abdominal distention because in organic abdominal distention there both total volume and abdominal content increase and cephalic displacement of the diaphragm occurs (30).
However, questions have arisen because neither patients with diarrhea-predominant IBS nor patients with only bloating were included in these studies making it difficult to generalize these concepts to all patients.
Recently the same group presented a similar study (32) with the intention of establishing the role of the diaphragm in abdominal distension. The study compared healthy adults with patients who suffer from abdominal distension. After introducing gas into the bowels of the patients their abdominal circumferences were measured and the muscles of the abdominal wall and the diaphragm were evaluated electromyographically. Paradoxically, the study demonstrated that significantly greater distention results from contraction of the diaphragm and from internal oblique muscle relaxation (32). The interesting aspect of this conclusion is that it opens up the possibility of new treatments based on correction of inappropriate diaphragm contraction with bio-feedback techniques to prevent anterior protrusion of the abdominal wall as another way of handling bloating (32, 33).
5. The role of the intestinal microbiota
The notion that there may be alterations of the intestinal microbiota patients with IBS and bloating is based on many observations. First, it was proposed that bacterial fermentation of undigested carbohydrates increases production of short-chain fatty acids and gases such as carbon dioxide, hydrogen and methane. More recently it has been demonstrated that in IBS patients the microbiota is altered and propionic acid production is increased. These patients show significant increases in Lactobacillus and Veillonella. It has also been shown that the production of acetic and propionic acid is related to presence of greater numbers and intensity of symptoms such as abdominal pain, bloating, and changes in bowel habits resulting in decreased quality of life (34, 35). Another series shows how the presence of ruminococcus torques is related to greater severity of IBS symptoms (36). Increased gas production in patients with IBS and bloating has been demonstrated by x rays which show that these patients contain higher gas volumes than do control patients (37). Similarly, other evaluations have shown that the quantity of gas produced by IBS patients is greater than that produced by control patients (38). This is in contrast to the reports previously mentioned according to which the important factors in this disorder are gas transit and alterations in sensitivity.
Small intestinal bacterial overgrowth (SIBO) is a clinical condition caused by excessive numbers of bacteria in the small intestine. It is characterized by symptoms such as diarrhea, abdominal pain and bloating which could be associated with excess gas due to increased production from bacterial fermentation in the gut (39). One of the most debated, controversial and interesting arguments is about the relationship of the intestinal microbiota with the genesis of SIBO and IBS (40, 41). The controversy begins with diagnosis, even though the method used is considered to be the gold standard. A bacterial count greater than 10 x 5 colony-forming units (CFUs)/Ml in a culture of jejunal aspirate are used. However, this methods limitations in terms of difficulty of obtaining samples, its invasive character, and problems of contamination and maintaining anaerobic conditions have led to considerable dispute about its use (42). A breath test such as the lactulose hydrogen breath test (LHBT) has been developed for evaluation of SIBO. It uses the carbohydrate metabolism of bacterial enzymes.
Dr. Pimentel´s group insists that there is a relationship between SIBO and IBS. In a very interesting editorial (43) based on further research, they support this theory with proper evidence and go on to propose a modification of Kochs postulates to establish the relationship between these two conditions and their genesis. They found that 78% of 202 IBS patients tested positive for LHBT suggesting that they have SIBO. They also found significant improvement of symptoms including abdominal pain, bloating and diarrhea when they treated SIBO with antibiotics. Patients Romes criteria changed from positive to negative (44). Other similar experiences with treatment support this association (45-47), however this does not totally resolve this controversy because doubts remain about the effectiveness of diagnostic methods for SIBO (48, 49). The prevalence of SIBO among IBS patients varies (49) plus general conceptual, epidemiological and therapeutic factors still need to be clarified (41, 50).
6. The role of food
At least two mechanism in which food generates bloating have been recognized: intolerance and hypersensitivity. Intolerance occurs in cases of fatty food, difficult to digest carbohydrates such as wheat and corn, non-absorbable sugars found in soft drinks, insoluble fiber, lactose in dairy products and vegetables such as cabbage and cauliflower. These foods can influence generation of symptoms in the gastrointestinal tract through many channels including activation of mechanoreceptors by their volume and physical properties and activation of chemoreceptors. Similarly, non-absorbable components can produce effects through osmotic action and fermentation in the colon (51-53).
On the other hand hypersensitivity activates the immune system through allergic phenomena and inflammation of the intestinal mucosa (54-56). As a practical consequence, it is not superfluous to mention here the importance of restricting consumption of these foods as a part of managing these patients.
7. Motor alterations
The role of gastrointestinal motility
If the important role that intestinal transit plays has been previously mentioned, attention is now being directed to the presence of specific alterations of the gastric motor function and their relationship with bloating. Gastroparesis is a condition in which this symptom is commonly observed and in which it often affects patients quality of life and requires therapeutic care (57).
The role of anorectal functioning
This aspect of the bloating´s pathophysiology has not been considered to be very relevant, but has generated interest due to observed alterations of the anorectal function especially in patients with constipation. This type of patient has been found to required prolonged times for rectal balloon expulsion and is a predictor of abdominal distension, which suggests that the ineffective evacuation of the gas and the stools with the extended rectal balloon expulsion which might be a mechanism related to bloating (58).
None of these observations can be looked at outside of the context of patients with functional digestive disorders for the genesis of which motor alterations are extremely important.
TREATMENT
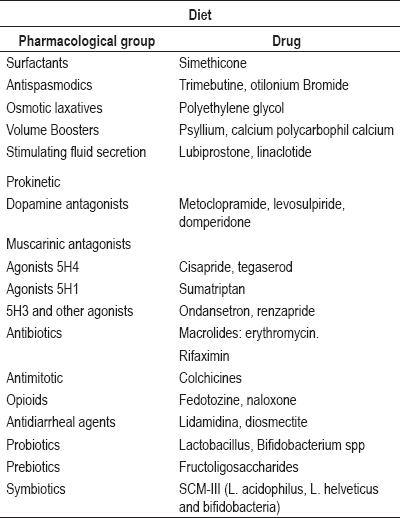
A general overview of current treatment for bloating shows that there are a great variety of options. A recent review shows detailed possibilities ranging from management of bloating with diet to the use of probiotics, surfactants such as simethicone, antispasmodics such as trimebutine, and otilonium bromide, osmotic laxatives (bulking), stimulation of fluid secretion, lubiprostone, prokinetics., antibiotics, and prebiotics (59)(See Table 2).
Table 2. Bloating and abdominal distention: treatment.
There are great expectations regarding the results of the Barcelona groups use of biofeedback to correct inappropriate diaphragm contractions and to prevent protrusion of the anterior abdominal wall as another way to manage bloating (32, 33).
It is important to remember that the handling of this complaint is part of the general context of a patient with a digestive functional disorder and requires contemplation of the patient in her/his environment as well as use of standardized management guidelines for appropriate approaches to the patient (60).
CONCLUSIONS
In this review of pathophysiological concepts related to the common complaints in patients with digestive functional disorders such as bloating and abdominal distension we have insisted on maintaining the linguistic difference between the two terms: bloating for the symptom and abdominal distension for the sign. We reviewed the various mechanisms in relation to production and handling of intestinal gas, transit and motor alterations, sensorial responses and visceral somatic responses. We particularly highlighted abdomino-phrenic dysfunction. We also analyzed the role of intestinal microbiota in the pathophysiology of bloating with special emphasis on the controversial role of SIBO. Finally, we included some considerations related to food and a panoramic vision of management of bloating.
REFERENCES
1. Choung RS, Locke GR. Epidemiology of IBS. Gastroenterol Clin North Am 2011; 40: 1-10.
2. Drossman DA. The functional gastrointestinal disorders and the Rome III process. Gastroenterology 2006; 130: 1377-90.
3. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional Bowel Disorders. Gastroenterology 2006; 130: 1480-91.
4. Schmulson M. Algoritmos de la Fundación de Roma para diagnóstico de síntomas gastrointestinales comunes en español. Rev Gastroenterolog Mex 2010; 75: 445-516.
5. Houghton LA, Lea R, Agrawal A, et al. Relationship of abdominal bloating to distension in irritable bowel syndrome and effect of bowel habit. Gastroenterology 2006; 131: 1003-1010.
6. Jiang X, Locke GR, 3rd, Choung RS, et al. Prevalence and risk factors for abdominal bloating and visible distension: a population based study. Gut 2008; 57: 756-763.
7. Agrawal A, Whorwell PJ. Review article: abdominal Bloating and distension in functional gastrointestinal disorders- epidemiology and exploration of possible mechanisms Aliment Pharmacol Ther 2008; 27: 2-1.
8. Chang L, Lee OY, Naliboff B, Schmulson M, Mayer EA. Sensation of bloating and visible abdominal distension in patients with irritable bowel syndrome. Am J Gastroenterol 2001; 96: 3341-7.
9. Talley NJ, Dennis EH, Schettler-Duncan EA, et al. Overlapping upper and lower gastrointestinal symptoms in irritable bowel syndrome patients with constipation or diarrhea. Am J Gastroenterol 2003; 98: 2454-9.
10. Tanaka Y, Kanazawa M, Fukudo S, Drossman DA. Biopsychosocial model of Irritable Bowel Syndrome. J Neurogastroenterol Motil 2011; 17: 131-139.
11. Drossman DA. Abuse, Trauma, and GI Illness: Is there a Link? Am J Gastroenterol 2011; 106: 14-25.
12. Song JY, Merskey H, Sullivan S. Anxiety and depression in patients with abdominal bloating. Can J Psychiatry 1993; 38: 475-9.
13. Zar S, Benson MJ, Kumar D. Review article: bloating in functional bowel disorders, Aliment Pharmacol Ther 2002; 16: 1867-1876.
14. Accarino A, Perez F, Azpiroz F, et al. Intestinal gas and bloating: effect of prokinetic stimulation. Am J Gastroenterol 2008; 103: 2036-2042.
15. Serra J, Azpiroz F, Malagelada JR. Impaired transit and tolerance of intestinal gas in the irritable bowel syndrome. Gut 2001; 48: 14-19.
16. Salvioli B, Serra J, Azpiroz F, Malagelada JR. Impaired small bowel gas propulsion in patients with bloating during intestinal lipid infusion. Am J Gastroenterol 2006; 101: 1853-7.
17. Agrawal A, Houghton LA, Reilly B, Morris J, Whorwell PJ. Bloating and distension in irritable bowel syndrome: the role of gastrointestinal transit. Am J Gastroenterol 2009; 104: 1998-2004.
18. Hernando-Harder AC, Serra J, Azpiroz F, Milà M, Aguadé S, Malagelada C, Tremolaterra F, Villoria A, Malagelada JR. Colonic responses to gas loads in subgroups of patients with abdominal bloating. Am J Gastroenterol 2010; 105: 876-82.
19. Zhou Q. Verne GN. New insights into visceral hypersensitivityclinical implications in IBS. Nat Rev Gastroenterol Hepatol 2011; 8: 349-355.
20. Azpiroz F. Gastrointestinal perception: pathophysiological implications. Neurogastroenterol Motil 2002; 14: 1-11.
21. Iovino P, Azpiroz F, Domingo E, et al. The sympathetic nervous system modulates perception and reflex responses to gut distension in humans. Gastroenterology 1995; 108: 680-6.
22. Azpiroz F, Malagelada JR. The Pathogenesis of Bloating and Visible Distension in Irritable Bowel Syndrome. Gastroenterol Clin N Am 2005; 34: 257-269.
23. Accarino AM, Azpiroz F, Malagelada JR. Attention and distraction: effects on gut perception. Gastroenterology 1997; 113:415-22.
24. Agrawal A, Houghton LA, Lea R, Morris J, Reilly B, Whorwell PJ. Bloating and Distension in Irritable Bowel Syndrome: The Role of Visceral Sensation. Gastroenterology 2008; 134: 1882-9.
25. Houghton LA. Bloating in constipation: Relevance of intraluminal gas handling. Best Practice & Research Clinical Gastroenterology 2011; 25: 141-150.
26. McManis PG, Newall D, Talley NJ. Abdominal wall muscle activity in irritable bowel syndrome with bloating. Am J Gastroenterol 2001; 96: 1139-1142.
27. Villoria A, Azpiroz F, Soldevilla A, et al. Abdominal accommodation: a coordinated adaptation of the abdominal wall to its content. Am J Gastroenterol 2008; 103: 2807-2815.
28. Tremolaterra F, Villoria A, Azpiroz F, et al. Impaired viscerosomatic reflexes and abdominal-wall dystony associated with bloating. Gastroenterology 2006; 130: 1062-1068.
29. Perez F, Accarino A, Azpiroz F, et al. Gas distribution within the human gut: effect of meals. Am J Gastroenterol 2007; 102: 842-849.
30. Accarino A, Perez F, Azpiroz F, Quiroga S, Malagelada JR. Abdominal distension results from caudo-ventral redistribution of contents. Gastroenterology 2009; 136: 1544-51.
31. Simrén M. Bloating and abdominal distension: not so poorly understood anymore! Gastroenterology 2009; 136: 1487-90.
32. Villoria A, Azpiroz F, Burri E, Cisternas D, Soldevilla A, Malagelada JR. Abdomino-phrenic dyssynergia in patients with abdominal bloating and distension. Am J Gastroenterol 2011; 106: 815-9.
33. Burri E, Azpiroz F, Hernández C. Biofeedback treatment of abdominal distention: a proof-of-concept [abstr]. Gut, in press.
34. Tana C, Umesaky Y, Imakoa A, Handa T, Kanazawa M, Fukudo S. Altered profiles of intestinal microbiota and organic acids may be the origin of symptoms in irritable bowel syndrome. Neurogastroenterol Motil 2010; 22: 512-515.
35. Malinen E, Rinttila T, Kajander K, Matto J, et al. Analysis of the fecal microbiota of irritable bowel syndrome patients and healthy controls with real-time PCR. Am J Gastroenterol 2005; 100: 373-382.
36. Malinen E, Krogius-Kurikka L, Lyra A, Nikkila J. Association of symptoms with gastrointestinal microbiota in irritable bowel syndrome. World J Gastroenterol 2010; 16: 4532-4540.
37. Koide A, Yamaguchi T, Odaka T. Quantitative analysis of bowel gas using plain abdominal radiograph in patients with irritable bowel syndrome. Am J Gastroenterol 2000; 95: 1735-41.
38. King TS, Elia M, Hunter JO. Abnormal colonic fermentation in irritable bowel syndrome. Lancet 1998; 352: 1187-9.
39. Vanner S. The small intestinal bacterial overgrowth. Irritable bowel syndrome hypothesis: implications for treatment. Gut 2008; 57: 1315-1321.
40. Park H. The Role of Small Intestinal Bacterial Overgrowth in the Pathophysiology of Irritable Bowel Syndrome. J Neurogastroenterol Motil 2010; 16: 1-3.
41. Spiegel BM. Questioning the bacterial overgrowth hypothesis of irritable bowel syndrome: an epidemiologic and evolutionary perspective. Clin Gastroenterol Hepatol 2011; 9: 461-9.
42. Shah ED, Basseri RJ, Chong K, Pimentel M. Abnormal breath testing in IBS: a meta-analysis. Dig Dis Sci 2010; 55: 2441-9.
43. Pimentel M. Evaluating a Bacterial Hypothesis in IBS Using a Modification of Kochs Postulates: Part 1. Am J Gastroenterol. 2010; 105: 718-21.
44. Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome: a double-blind, randomized, placebo controlled study. Am J Gastroenterol 2003; 98: 412-9.
45. Pimentel M, Park S, Kane SV et al. The effect of a nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel syndrome: a randomized trial. Ann Intern Med 2006; 145: 557-63.
46. Lembo A, Zakko SF, Ferreira NL, et al. Rifaximin for the treatment of diarrhea-associated irritable bowel syndrome: short term treatment leading to long term sustained response [abstr]. Gastroenterology 2008; 134: A545.
47. Sharara AI, Aoun E, Abdul-Baki H et al. A randomized double-blind placebo-controlled trial of rifaximin in patients with abdominal bloating and flatulence. Am J Gastroenterol 2006; 101: 326-33.
48. Connolly L, Chang L. Combined orocecal scintigraphy and lactulose hydrogen breath testing demonstrate that breath testing detects orocecal transit, not small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Gastroenterology 2011; 141: 1118-21.
49. Ford AC, Spiegel BM, Talley NJ, Moayyedi P. Small intestinal bacterial overgrowth in irritable bowel syndrome: systematic review and meta-analysis. Clin Gastroenterol Hepatol 2009; 7: 1279-86.
50. Eswaran S, Tack J, Chey WD. Food: the forgotten factor in the irritable bowel syndrome. Gastroenterol Clin North Am 2011; 40: 141-62.
51. Marteau P, Flourié B. Tolerance to low-digestible carbohydrates: symptomatology and methods. Br J Nutr 2001; 85 Suppl 1: S17-21.
52. Jellema P, Schellevis FG, van der Windt DA, Kneepkens CM, van der Horst HE. Lactose malabsorption and intolerance: a systematic review on the diagnostic value of gastrointestinal symptoms and self-reported milk intolerance. QJM 2010; 103: 555-72.
53. Lied GA, Lillestøl K, Lind R, Valeur J, Morken MH, Vaali K, Gregersen K, Florvaag E, Tangen T, Berstad A. Perceived food hypersensitivity: a review of 10 years of interdisciplinary research at a reference center. Scand J Gastroenterol 2011; 46: 1169-78.
54. Verdu EF. Editorial: Can gluten contribute to irritable bowel syndrome? Am J Gastroenterol 2011; 106: 516-8.
55. Biesiekierski JR, Newnham ED, Irving PM, Barrett JS, Haines M, Doecke JD, Shepherd SJ, Muir JG, Gibson PR. Gluten causes gastrointestinal symptoms in subjects without celiac disease: a double-blind randomized placebo-controlled trial. Am J Gastroenterol 2011; 106: 508-14.
56. Hasler WL, Wilson LA, Parkman HP, Nguyen L, Abell TL, Koch KL, Pasricha PJ, Snape WJ, Farrugia G, Lee L, Tonascia J, Unalp-Arida A, Hamilton F; NIDDK Gastroparesis Clinical Research Consortium (GpCRC). Bloating in gastroparesis: Severity, impact and associated factors. Am J Gastroenterol 2011; 106(8): 1492-502.
57. Shim L, Prott G, Hansen RD, Simmons LE, Kellow JE, Malcolm A. Prolonged balloon expulsion is predictive of abdominal distension in bloating. Am J Gastroenterol 2010; 105(4): 883-7.
58. Schmulson M, Chang L. Review article: the treatment of functional abdominal bloating and distension Aliment Pharmacol Ther 2011; 33: 1071-86.
59. World Gastroenterology Organization Global GuidelineIrritable Bowel Syndrome: A Global Perspective. April 20, 2009. http://www.worldgastroenterology.org/irritablebowelsyndrome.html
1. Choung RS, Locke GR. Epidemiology of IBS. Gastroenterol Clin North Am 2011; 40: 1-10. [ Links ]
2. Drossman DA. The functional gastrointestinal disorders and the Rome III process. Gastroenterology 2006; 130: 1377-90. [ Links ]
3. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional Bowel Disorders. Gastroenterology 2006; 130: 1480-91. [ Links ]
4. Schmulson M. Algoritmos de la Fundación de Roma para diagnóstico de síntomas gastrointestinales comunes en español. Rev Gastroenterolog Mex 2010; 75: 445-516. [ Links ]
5. Houghton LA, Lea R, Agrawal A, et al. Relationship of abdominal bloating to distension in irritable bowel syndrome and effect of bowel habit. Gastroenterology 2006; 131: 1003-1010. [ Links ]
6. Jiang X, Locke GR, 3rd, Choung RS, et al. Prevalence and risk factors for abdominal bloating and visible distension: a population based study. Gut 2008; 57: 756-763. [ Links ]
7. Agrawal A, Whorwell PJ. Review article: abdominal Bloating and distension in functional gastrointestinal disorders- epidemiology and exploration of possible mechanisms Aliment Pharmacol Ther 2008; 27: 2-1. [ Links ]
8. Chang L, Lee OY, Naliboff B, Schmulson M, Mayer EA. Sensation of bloating and visible abdominal distension in patients with irritable bowel syndrome. Am J Gastroenterol 2001; 96: 3341-7. [ Links ]
9. Talley NJ, Dennis EH, Schettler-Duncan EA, et al. Overlapping upper and lower gastrointestinal symptoms in irritable bowel syndrome patients with constipation or diarrhea. Am J Gastroenterol 2003; 98: 2454-9. [ Links ]
10. Tanaka Y, Kanazawa M, Fukudo S, Drossman DA. Biopsychosocial model of Irritable Bowel Syndrome. J Neurogastroenterol Motil 2011; 17: 131-139. [ Links ]
11. Drossman DA. Abuse, Trauma, and GI Illness: Is there a Link? Am J Gastroenterol 2011; 106: 14-25. [ Links ]
12. Song JY, Merskey H, Sullivan S. Anxiety and depression in patients with abdominal bloating. Can J Psychiatry 1993; 38: 475-9. [ Links ]
13. Zar S, Benson MJ, Kumar D. Review article: bloating in functional bowel disorders, Aliment Pharmacol Ther 2002; 16: 1867-1876. [ Links ]
14. Accarino A, Perez F, Azpiroz F, et al. Intestinal gas and bloating: effect of prokinetic stimulation. Am J Gastroenterol 2008; 103: 2036-2042. [ Links ]
15. Serra J, Azpiroz F, Malagelada JR. Impaired transit and tolerance of intestinal gas in the irritable bowel syndrome. Gut 2001; 48: 14-19. [ Links ]
16. Salvioli B, Serra J, Azpiroz F, Malagelada JR. Impaired small bowel gas propulsion in patients with bloating during intestinal lipid infusion. Am J Gastroenterol 2006; 101: 1853-7. [ Links ]
17. Agrawal A, Houghton LA, Reilly B, Morris J, Whorwell PJ. Bloating and distension in irritable bowel syndrome: the role of gastrointestinal transit. Am J Gastroenterol 2009; 104: 1998-2004. [ Links ]
18. Hernando-Harder AC, Serra J, Azpiroz F, Milà M, Aguadé S, Malagelada C, Tremolaterra F, Villoria A, Malagelada JR. Colonic responses to gas loads in subgroups of patients with abdominal bloating. Am J Gastroenterol 2010; 105: 876-82. [ Links ]
19. Zhou Q. Verne GN. New insights into visceral hypersensitivityclinical implications in IBS. Nat Rev Gastroenterol Hepatol 2011; 8: 349-355. [ Links ]
20. Azpiroz F. Gastrointestinal perception: pathophysiological implications. Neurogastroenterol Motil 2002; 14: 1-11. [ Links ]
21. Iovino P, Azpiroz F, Domingo E, et al. The sympathetic nervous system modulates perception and reflex responses to gut distension in humans. Gastroenterology 1995; 108: 680-6. [ Links ]
22. Azpiroz F, Malagelada JR. The Pathogenesis of Bloating and Visible Distension in Irritable Bowel Syndrome. Gastroenterol Clin N Am 2005; 34: 257-269. [ Links ]
23. Accarino AM, Azpiroz F, Malagelada JR. Attention and distraction: effects on gut perception. Gastroenterology 1997; 113:415-22. [ Links ]
24. Agrawal A, Houghton LA, Lea R, Morris J, Reilly B, Whorwell PJ. Bloating and Distension in Irritable Bowel Syndrome: The Role of Visceral Sensation. Gastroenterology 2008; 134: 1882-9. [ Links ]
25. Houghton LA. Bloating in constipation: Relevance of intraluminal gas handling. Best Practice & Research Clinical Gastroenterology 2011; 25: 141-150. [ Links ]
26. McManis PG, Newall D, Talley NJ. Abdominal wall muscle activity in irritable bowel syndrome with bloating. Am J Gastroenterol 2001; 96: 1139-1142. [ Links ]
27. Villoria A, Azpiroz F, Soldevilla A, et al. Abdominal accommodation: a coordinated adaptation of the abdominal wall to its content. Am J Gastroenterol 2008; 103: 2807-2815. [ Links ]
28. Tremolaterra F, Villoria A, Azpiroz F, et al. Impaired viscerosomatic reflexes and abdominal-wall dystony associated with bloating. Gastroenterology 2006; 130: 1062-1068. [ Links ]
29. Perez F, Accarino A, Azpiroz F, et al. Gas distribution within the human gut: effect of meals. Am J Gastroenterol 2007; 102: 842-849. [ Links ]
30. Accarino A, Perez F, Azpiroz F, Quiroga S, Malagelada JR. Abdominal distension results from caudo-ventral redistribution of contents. Gastroenterology 2009; 136: 1544-51. [ Links ]
31. Simrén M. Bloating and abdominal distension: not so poorly understood anymore! Gastroenterology 2009; 136: 1487-90. [ Links ]
32. Villoria A, Azpiroz F, Burri E, Cisternas D, Soldevilla A, Malagelada JR. Abdomino-phrenic dyssynergia in patients with abdominal bloating and distension. Am J Gastroenterol 2011; 106: 815-9. [ Links ]
33. Burri E, Azpiroz F, Hernández C. Biofeedback treatment of abdominal distention: a proof-of-concept [abstr]. Gut, in press. [ Links ]
34. Tana C, Umesaky Y, Imakoa A, Handa T, Kanazawa M, Fukudo S. Altered profiles of intestinal microbiota and organic acids may be the origin of symptoms in irritable bowel syndrome. Neurogastroenterol Motil 2010; 22: 512-515. [ Links ]
35. Malinen E, Rinttila T, Kajander K, Matto J, et al. Analysis of the fecal microbiota of irritable bowel syndrome patients and healthy controls with real-time PCR. Am J Gastroenterol 2005; 100: 373-382. [ Links ]
36. Malinen E, Krogius-Kurikka L, Lyra A, Nikkila J. Association of symptoms with gastrointestinal microbiota in irritable bowel syndrome. World J Gastroenterol 2010; 16: 4532-4540. [ Links ]
37. Koide A, Yamaguchi T, Odaka T. Quantitative analysis of bowel gas using plain abdominal radiograph in patients with irritable bowel syndrome. Am J Gastroenterol 2000; 95: 1735-41. [ Links ]
38. King TS, Elia M, Hunter JO. Abnormal colonic fermentation in irritable bowel syndrome. Lancet 1998; 352: 1187-9. [ Links ]
39. Vanner S. The small intestinal bacterial overgrowth. Irritable bowel syndrome hypothesis: implications for treatment. Gut 2008; 57: 1315-1321. [ Links ]
40. Park H. The Role of Small Intestinal Bacterial Overgrowth in the Pathophysiology of Irritable Bowel Syndrome. J Neurogastroenterol Motil 2010; 16: 1-3. [ Links ]
41. Spiegel BM. Questioning the bacterial overgrowth hypothesis of irritable bowel syndrome: an epidemiologic and evolutionary perspective. Clin Gastroenterol Hepatol 2011; 9: 461-9. [ Links ]
42. Shah ED, Basseri RJ, Chong K, Pimentel M. Abnormal breath testing in IBS: a meta-analysis. Dig Dis Sci 2010; 55: 2441-9. [ Links ]
43. Pimentel M. Evaluating a Bacterial Hypothesis in IBS Using a Modification of Kochs Postulates: Part 1. Am J Gastroenterol. 2010; 105: 718-21. [ Links ]
44. Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome: a double-blind, randomized, placebo controlled study. Am J Gastroenterol 2003; 98: 412-9. [ Links ]
45. Pimentel M, Park S, Kane SV et al. The effect of a nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel syndrome: a randomized trial. Ann Intern Med 2006; 145: 557-63. [ Links ]
46. Lembo A, Zakko SF, Ferreira NL, et al. Rifaximin for the treatment of diarrhea-associated irritable bowel syndrome: short term treatment leading to long term sustained response [abstr]. Gastroenterology 2008; 134: A545. [ Links ]
47. Sharara AI, Aoun E, Abdul-Baki H et al. A randomized double-blind placebo-controlled trial of rifaximin in patients with abdominal bloating and flatulence. Am J Gastroenterol 2006; 101: 326-33. [ Links ]
48. Connolly L, Chang L. Combined orocecal scintigraphy and lactulose hydrogen breath testing demonstrate that breath testing detects orocecal transit, not small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Gastroenterology 2011; 141: 1118-21. [ Links ]
49. Ford AC, Spiegel BM, Talley NJ, Moayyedi P. Small intestinal bacterial overgrowth in irritable bowel syndrome: systematic review and meta-analysis. Clin Gastroenterol Hepatol 2009; 7: 1279-86. [ Links ]
50. Eswaran S, Tack J, Chey WD. Food: the forgotten factor in the irritable bowel syndrome. Gastroenterol Clin North Am 2011; 40: 141-62. [ Links ]
51. Marteau P, Flourié B. Tolerance to low-digestible carbohydrates: symptomatology and methods. Br J Nutr 2001; 85 Suppl 1: S17-21. [ Links ]
52. Jellema P, Schellevis FG, van der Windt DA, Kneepkens CM, van der Horst HE. Lactose malabsorption and intolerance: a systematic review on the diagnostic value of gastrointestinal symptoms and self-reported milk intolerance. QJM 2010; 103: 555-72. [ Links ]
53. Lied GA, Lillestøl K, Lind R, Valeur J, Morken MH, Vaali K, Gregersen K, Florvaag E, Tangen T, Berstad A. Perceived food hypersensitivity: a review of 10 years of interdisciplinary research at a reference center. Scand J Gastroenterol 2011; 46: 1169-78. [ Links ]
54. Verdu EF. Editorial: Can gluten contribute to irritable bowel syndrome? Am J Gastroenterol 2011; 106: 516-8. [ Links ]
55. Biesiekierski JR, Newnham ED, Irving PM, Barrett JS, Haines M, Doecke JD, Shepherd SJ, Muir JG, Gibson PR. Gluten causes gastrointestinal symptoms in subjects without celiac disease: a double-blind randomized placebo-controlled trial. Am J Gastroenterol 2011; 106: 508-14. [ Links ]
56. Hasler WL, Wilson LA, Parkman HP, Nguyen L, Abell TL, Koch KL, Pasricha PJ, Snape WJ, Farrugia G, Lee L, Tonascia J, Unalp-Arida A, Hamilton F; NIDDK Gastroparesis Clinical Research Consortium (GpCRC). Bloating in gastroparesis: Severity, impact and associated factors. Am J Gastroenterol 2011; 106(8): 1492-502. [ Links ]
57. Shim L, Prott G, Hansen RD, Simmons LE, Kellow JE, Malcolm A. Prolonged balloon expulsion is predictive of abdominal distension in bloating. Am J Gastroenterol 2010; 105(4): 883-7. [ Links ]
58. Schmulson M, Chang L. Review article: the treatment of functional abdominal bloating and distension Aliment Pharmacol Ther 2011; 33: 1071-86. [ Links ]
59. World Gastroenterology Organization Global GuidelineIrritable Bowel Syndrome: A Global Perspective. April 20, 2009. http://www.worldgastroenterology.org/irritablebowelsyndrome.html [ Links ]

