











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Motor learning is a key adaptive mechanism for solving problems of daily life that is used to maintain known behavioral capacities and to learn new skills. 1 Human motor control requires a learning and training process known as feedback, in which the nervous system makes a constant comparison between the desired value and the value it receives in real time from the environment. 2-4
Hence, the use of a system that feeds back in a positive or negative way the execution of a motor gesture could modulate this movement, which would favor learning. 1-5 In this sense, there is a series of techniques and tools that provide feedback on the movement performed and influence its control. 3,6 These tools, used both in physical rehabilitation and in sports training, are associated mainly to visual, tactile, proprioceptive and auditory stimuli; the latter has not been studied sufficiently. 3
Rosati et al.5 used visual and auditory feedback together, and demonstrated that they would help improve performance and learning in the execution of exercises with the upper limbs. On the other hand, Portnoy et al.7 demonstrated the effectiveness of auditory feedback compared to kinesthetic learning during the execution of a motor gesture, a result that has not been reported in other studies focused on learning the movement generated with this type of intervention.
Furthermore, an objective evaluation to measure motor control of the upper limb and, specifically, of glenohumeral movement requires sophisticated systems that, in general, are inefficient for clinical practice, since they are time-consuming, costly and may require a laboratory. 8 Therefore, several studies 8-15 highlight the benefits of accelerometers and inertial sensors as inexpensive and easy to use methods that provide reliable and fast data.
Root mean square (RMS) is a measure of central tendency 16 that is used in various studies to measure the vibration of different segments of the human body in the context of motion analysis. 13,14,17,18 Similarly, Körver et al.8 have proposed to study clinical shoulder variables with accelerometry and to include acromion-sensor distance (ASD), body mass index (BMI) and sex within the analyses.
With this in mind, the objective of this research is to determine variations in glenohumeral movement control through learning in young adults exposed to an auditory feedback system, while performing object translation tasks classified by difficulty level.
Materials and methods
Design
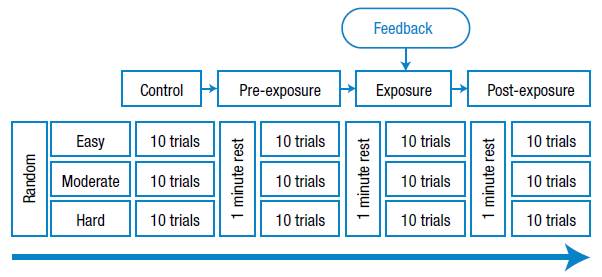
Cross-sectional study with time series evaluations including four measurement stages in the same group: control, pre-exposure, exposure (with auditory feedback) and post-exposure. Figure 1 presents the four stages of the research, which consisted of the tasks that were executed, classified according to the difficulty level. The third stage (exposure) corresponds to that implemented with the auditory feedback system.
Participants
The sample consisted of 45 young adults (22.78+3.45 years) of both sexes (23 men and 22 women) with a BMI of 27.30+5.31 and an ASD of 29.86+2.07cm. The participants, who came from the Araucanía region of Chile, agreed to participate freely in the study by signing an informed consent form and were selected in a non-probabilistic, intentional manner. Sample size was determined using the method proposed by Hulley et al.19
The inclusion criteria were: being a university student over 18 years of age and having access to the evaluation during the period of execution (six months) as planned. The exclusion criteria were: having a history of painful shoulder conditions, having a pathology directly or indirectly associated with the function of the upper limb, and having hearing impairment or sensory processing disorders. In order to confirm the suitability for the study, each participant took a brief recognition test of the musical notes that would be used in the feedback, during which they were requested to classify the notes as low-pitched or high-pitched; an error of 20% was considered an exclusion criterion.
The measurement protocol was approved by the Institutional Ethics Committee of the Universidad de Santiago de Chile through Minutes No. 576 of October 17, 2016 and was developed in accordance with the ethical principles of the Declaration of Helsinki. 20
Measurements
During the pilot study, an auditory feedback system based on accelerometry was implemented, since these types of sensors are widely used in various electronic devices, which would favor transfer and massification.
The sensor used was an analog accelerometer (Freescale Semiconductor® model MMA7361, USA) that was connected to an electronic board (Arduino® model UNO, Italy), and communicated to a laptop computer (ASUS model X455L, China) via a serial port; the data was collected using Matlab® software, version R2012b (USA). The acceleration sensor was adhered to the skin with double-sided tape at the midpoint of the triangle formed by the olecranon, lateral epicondyle and medial epicondyle of the humerus while the elbow was in 90° flexion. 8,9,21
Accelerometer measurement data were obtained throughout four consecutive study stages. Based on previous research 15, a protocol adapted to the objective of the study was planned, including 10 trials for each difficulty level of the task, divided into blocks of 40 seconds with a pause of 1 minute, totaling 120 trials per participant.
In order to obtain the accelerometry RMS and the task execution speed (TES), the digitized raw data were processed. Firstly, the data were processed using a 4th-order Butterworth low pass digital filter with a cutoff frequency of 10Hz. Secondly, to eliminate the effects of the sensor position, the signal was centered at zero and a copy of it, softened with the same type of filter, was subtracted with a cutoff frequency of 0.1Hz. 22 Then, the RMS was calculated for the resulting signal and, finally, it was multiplied by the force of gravity and the acceleration obtained in velocity was integrated.
Intervention
The intervention consisted of four stages which were distributed as follows:
Control: The participants were explained that the vibration or position of their arm during movement was going to be measured. To this end, they were asked to perform the easy, moderate and hard tasks. Pre-exposure: The procedure carried out in the control stage was repeated.
Exposure (with auditory feedback): Participants were told that the vibrations or position of their arm during movement was going to be measured while listening to a musical note (A, B, C, D, E, F and G). The musical note emitted, which depends on the vibration or position of the arm, would be high-pitched at higher vibration and low-pitched at lower vibration, so the instruction was to perform the tasks by making the system play low-pitched notes. Post-exposure: The procedure carried out in the control stage was repeated.
In order to classify the tasks performed in each of the stages according to difficulty, the Flexilevel Scale of Shoulder Function was adapted taking into account the materials available in the evaluation laboratory. This scale consists of three subsets of items (tasks) that allow the general classification of different levels of shoulder function. 23 In this way, the tasks were classified as:
Easy: The participants were seated and had to touch the earlobe of the same side of their dominant arm, and then return to the initial position. Moderate: The participants were seated and required to move a 2kg dumbbell from a 19cm high footstool with the dominant arm, located 5cm from their side, to a 70cm table located 17cm in front of them, and then return to the initial position.
Hard: The participants were seated and required to move a 2kg dumbbell with the dominant arm from a table located 22cm in front of them to a 142cm shelf and then return to the initial position.
Procedure
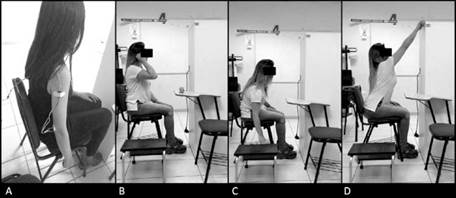
Each volunteer was assigned a date and time for the measurements. First, a brief interview was conducted to collect information on age, sex, and upper limb dominance. Then, body weight and height of the feet were obtained to calculate the BMI 24 by means of a mechanical patient weighing scale with a measuring rod (Detecto® model 339, USA; accuracy 0.1kg and 0.1cm). The accelerometer was then placed and the ASD was measured using the Sanny anthropometric tape (Brazil; accuracy 0.1cm) from the lateral border of the acromion to the midpoint of the sensor. 8,9 Finally, the evaluation was carried out using an accelerometer-based system, in four successive stages, where the order of the difficulty level was random (Figure 2).
Statistical analysis
The Statistical Package for the Social Sciences® (SPSS) version 23.0 was used for analysis. The data were subjected to the Shapiro-Wilk normality test. The Wilcoxon nonparametric test was used to identify differences in the means of the dependent variables; the Spearman ranges test was used to establish correlations according to the different tasks and stages of the study (between the variables RMS and TES; RMS and ASD; RMS and BMI); the point-biserial correlation was used for nonparametric correlation analysis of independent variables to determine the correlation between RMS and sex. In all cases, a significance level of p<0.05 was established.
Results
A significant decrease in RMS was observed during the exposure stage (Figure 3). Statistically significant differences were found between the pre-exposure and exposure stages (p<0.001), and between pre- exposure and post-exposure for the three task difficulty levels (Table 1). Statistically significant differences were compared using the Wilcoxon test. Data were expressed in mean and standard deviation.
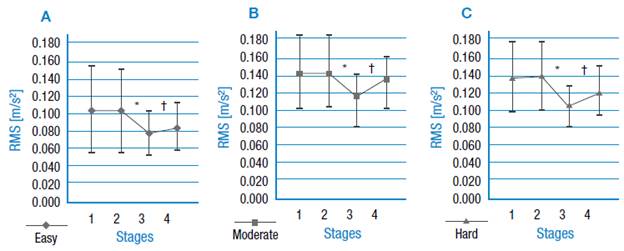
1: control stage; 2: pre-exposure stage; 3: exposure stage; 4: post-exposure stage. * represents statistically significant differences (p<0.01) between the pre-exposure and exposure stages. † represents statistically significant differences (p<0.01) between the pre-exposure and post-exposure stages. Source: Own elaboration.
Figure 3 Root Mean Square (mean) of the participants (n=45) according to the stage and difficulty of the task. A) trials associated with an easy task; B) trials associated with a task of moderate difficulty; C) trials associated with a hard task.
Table 1 Differences (mean) of the root mean square and the speed of execution of the task between the stages of the study and difficulty level of the task.
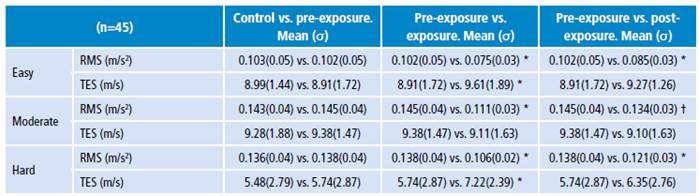
σ: standard deviation; RMS: raíz root mean square; TES: task execution speed.
* p<0.001
† p<0.01
Source: Own elaboration.
Regarding TES, a significant increase (p<0.001) in speed between the pre-exposure and exposure stages was identified for tasks classified as easy and hard (Figure 4). Statistically significant differences were compared using the Wilcoxon test.
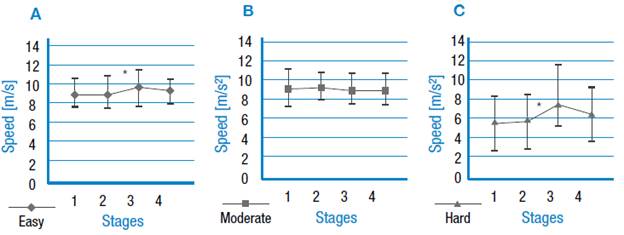
Source: Own elaboration.
Figure 4 Average execution speed of the participants (n=45) depending on the stage and difficulty of the task. A) trials associated with an easy task; B) trials associated with a task of moderate difficulty; C) trials associated with a difficult task. 1: control stage; 2: pre-exposure stage; 3: exposure stage; 4: post-exposure stage. * represents statistically significant differences (p<0.01) between the pre-exposure and exposure stages.
By correlating the RMS with its corresponding TES for each stage and task difficulty, it was found that in the post-exposure stage of the easy task there was a slightly significant inverse correlation (p=0.047), which also has a very small coefficient (r=-0.298), while the pre-exposure and exposure stages do not have statistically significant differences (Table 2). An inverse correlation between RMS and ASD was found in all the task difficulties and at all stages. A direct correlation between the RMS and BMI variables was observed in the control, pre-exposure and post-exposure stages for the easy and moderate tasks. In addition, an inverse correlation between RMS and sex was reported for all task and stage difficulties (Table 2). For the correlation between RMS and sex, point biserial correlation coefficient was used, where 0=female and 1=masculine.
Table 2 Correlations between the variables of the study, distributed by stage and difficulty level of the task.
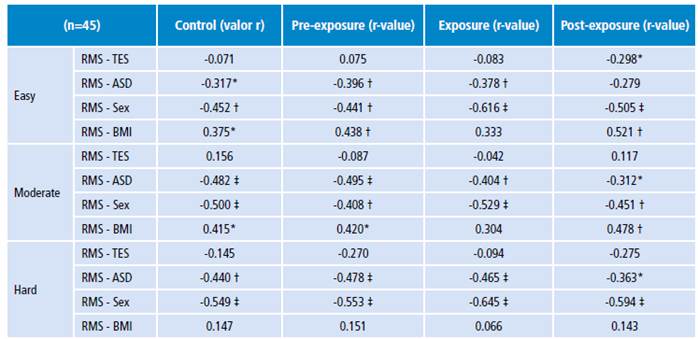
RMS: root mean square; TES: task execution speed; ASD: acromion-sensor distance; BMI: body mass index; r-value: correlation coefficient through Spearman rank correlation.
* p<0.05
† p<0.01
‡ p<0.001
Source: Own elaboration.
Discussion
The most relevant result of this research points to the existence of variations in the control of glenohumeral movement when implementing an auditory feedback system, which are manifested at all difficulty levels of the task.
Huang et al.15 report a direct correlation between the difficulty of a range task and the magnitude of the accelerometry signal vector. In this respect, our results indicate a higher RMS of accelerometry in the task of moderate difficulty, followed by the hard and the easy tasks, in that order. The task of moderate difficulty presented a greater tendency to leave the sagittal plane while the movement was being executed, which could have a direct impact on the RMS obtained. However, this variation could be the result of several factors such as the number of participants, so it would be advisable to expand the sample to find if the trend persists.
When comparing the RMS between the pre-exposure and exposure stages, statistically significant differences were found in the three task difficulties, so the intervention would be favorable for decreasing the RMS. This is interpreted as a better control of the glenohumeral movement due to a lower number of adjustments during performance. On the contrary, no significant differences were reported between the control and pre-exposure stages for RMS and TES, which would indicate that the execution of 10 trials in these stages does not modify the execution of the movement in the participants.
When evaluating the RMS between the pre-exposure and post-exposure stages, statistically significant differences were found in the three task difficulties; therefore, the intervention continues to produce variations in the post-exposure stage. This could be associated with a modification of the motor strategy after receiving auditory feedback 3, i.e., the intervention would contribute to motor learning in the participants.
With respect to TES, statistically significant differences were found in the easy and hard tasks with a tendency towards an increase in speed. In this regard, Sugamoto et al.25 state that rapid movements represent better the motor functionality of humans, as the speed of the movement determines the motor strategy used. Consequently, the findings of this study become useful information for future research on the subject, since the intervention would not slow down the movement.
An attempt was made to identify a possible correlation between RMS and TES, since a correlation between repetitive TES and muscle response was previously found 26; it could be assumed that a task performed at low speed is related to lower values of RMS. The results of this research showed that RMS decreases without the need for a slower execution of the task, which could indicate that the feedback used generates a better response in the participants.
In relation to the covariates analyzed, studies with similar evaluation procedures 8,9 identified ASD as a possible modifier of the accelerometry signal, which coincides with the results of this research, since RMS had an inverse correlation (p<0.05) with ASD. There was a lower RMS in the participants who had short humerus, a result that could indicate that the amplitude of the accelerometry signal decreases the closer the sensor is to the axis of motion. 8,9 The RMS correlated directly with the female sex, which would indicate a greater number of accommodations with respect to the trajectory of movement. Likewise, having a high BMI correlated with greater adjustment in men and women, a fact that could be linked to the physical-functional capacity of the participants. Although sex and BMI were related to RMS, no studies with similar characteristics were found to compare the results, so these variables should be addressed in future interventions.
The use of an objective measurement of low cost through accelerometers is one of the strengths of this study, since these sensors are found in most smartphones 27, thus turning into an opportunity to apply auditory feedback or other similar tools in these devices. Other elements that favor the internal validity of the measurements are the low difference obtained between the control and pre-exposure stages, the scarce time elapsed between the tasks, and their random order of execution.
One of the limitations was that the sensor used does not have the best quality in the market, which leads to a higher noise level; however, the used offline digital filtering processes helped to obtain the produced signal. Likewise, the weight of the transferred object according to the physical characteristics of the participants or sex was not considered. With all this in mind and considering the sample size, it is not possible to generalize the results of the study. However, new research could compare the results with a larger group of participants with different age ranges or even with a motor deficit.
In a practical context, this auditory feedback system is useful as a teaching-learning strategy for the control of glenohumeral movement during object translation tasks, which would support its use as a tool to choose exercises for the rehabilitation of function in the upper limbs. Another application that could result from this research is the use of auditory feedback as an intermediate stage between visual feedback and proprioceptive feedback, or it could even be used as a rehabilitation tool for people with visuomotor impairments and visual impairment. However, more research is needed in this field for its clinical application.
Conclusion
The use of an auditory feedback system in young adults without pathologies could favor learning and control of glenohumeral movement without reducing TES. This effect is maintained after feedback, so the use of this type of feedback system in healthy individuals could result in a useful strategy for the training of motor control of the shoulder.


