











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The knee is one of the most complex joint structures in the human body. It is composed of the tibiofemoral and patellofemoral joints1-4 and its formation involves both bone components (femur, tibia, and patella) and soft tissue components (synovial membrane, joint capsule, bursae, retinaculum, meniscus, and ligaments).
The movements of the knee occur in the tibiofemoral joint and are mainly flexion and extension, but there may also be internal and external rotation to a lesser extent.2,6,7 The range of motion for knee flexion is 130° to 140°; however, these values may increase or decrease depending on the position of the hip joint during knee movement.2,8
Currently, there are different diagnostic tests and specific exploratory maneuvers to assess the anatomic and functional characteristics of the knee joint complex. These tools are based on tests and clinical signs, and require the expertise of the physical therapist for a correct execution and interpretation of the results, and for a proper assessment of the integrity of the cartilage, muscles, menisci, ligament stability, etc.9
The functioning of the knee can be affected by pathologies of traumatic, degenerative, genetic, neurological, or autoimmune origin,10 the first two being the most common types. Depending on the type of injury, different intervention protocols should be implemented, using different techniques aimed at proprioceptive re-education to encourage the execution of reflex activities and activate and strengthen muscle groups to stabilize the joint and improve its muscle elasticity and joint thickness. These techniques are also useful for gait training and re-education of the sporting gesture.
Rehabilitation processes are based on protocols and clinical practice guidelines with therapeutic objectives that seek to potentiate joint motion through anisometric contractions that modify the length of the muscle.11-13 Also, to determine the progress of the interventions, multiple devices are available to measure variables such as angular position, angular velocities, force and torque in different joints of the body.14-17 However, these equipment are expensive and rehabilitation centers cannot afford them and must perform therapies in the traditional manner. Therefore, it is common that physical therapists do not have access to quantitative data that help them determine patients' progress during the different phases of rehabilitation.
Specifically, joint torque measurement is used to objectively determine patient progress as rehabilitation progresses15-17 and is used in therapeutic interventions for anterior cruciate ligament injuries,11,17 postoperative meniscectomy rehabilitations,16 lumbar injuries,15 among others. To this end, devices such as the Contrex18 and Human Norm19 systems are available on the market to monitor torque and allow the visualization of graphs that evidence the progress of this variable but, as mentioned above, they can be expensive and, in the Colombian case, they cost at least 10 times more than surface electromyography (sEMG) signal processing equipment.20,21
Isokinetic dynamometers are instruments that allow obtaining information on torque during knee flexion-extension movement and, this way, establish its angle and maximum peak, as well as muscle power, muscle balance, etc.; these results allow quantifying objectively the recovery of the patient.16,22-27 It should be noted that, despite its usefulness, the periodic collection of these data is limited due to high technology costs and, therefore, institutions prefer to use isometric dynamometers that have a lower cost but only allow measurements in static positions. This considerably limits the collection of relevant information for the implementation of rehabilitation processes.
On the other hand, sEMG signals are used as an alternative to estimate joint movements and the amount of force needed to perform a motor task,28 as well as to determine the state of the musculoskeletal or neuromuscular system,29-31 as they provide valuable information on the timing and relative intensity of muscle activity.32,33 These signals are measured with surface electrodes placed on the skin above the muscle group of interest.28,29,34 Currently, there are several low-cost sEMG sensors, which represents an advantage over other devices such as isokinetic dynamometers.
Given this scenario, the objective of the present work was to conduct a literature review on the use of sEMG signals as an alternative to calculate knee joint torque to objectively measure patients' progress during the different stages of rehabilitation of injuries in this joint.
Materials and methods
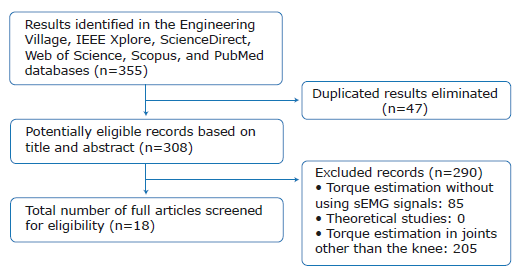
A literature review was conducted based on the Cochrane Collaboration handbook.35 The search was performed on the Engineering Village, IEEE Xplore, ScienceDirect, Web of Science, Scopus and PubMed databases using the following search strategy: years of publication: 1986 to 2018; type of publications: article and conference proceedings; language: English and Spanish; search equation: ("torque measurement" OR "torque estimation" OR "estimation of torque") AND (EMG OR sEMG OR electromyography OR electromyographic) AND Knee.
This review was based on the algorithms that have been developed to estimate knee joint torque through sEMG signals. It also considered how these algorithms can be used as an alternative to quantify the progress of patients during rehabilitation. To determine the search equation, MeSH terms that met the description required by the authors were established.
Publications in which sEMG signals were used to calculate knee joint torque were included. State-of-the-art reviews and references where torque was not measured using sEMG signals or which estimated torque in joints other than the knee were excluded. For information analysis, the current commercial value of isometric and isokinetic dynamometers in Colombia was considered.
355 records were retrieved, of which 47 were eliminated because they were duplicated. Exclusion and inclusion criteria were applied to the remaining 308 records, which led to eliminate 290 of them. Therefore, 18 publications were finally included (Figure 1).
Results
A total of 18 publications that describe, in a comparative way, how to estimate knee joint torque from sEMG signals were retrieved; the most relevant aspects are presented in Table 1. All the articles found were published in English and were original research works published in indexed journals and in memoirs of events.
Table 1 Torque estimation algorithms based on surface electromyography signals.
| Author/Year | Torque estimation strategy | Surface electromyography signal processing | Muscles used | Type of contraction | Number of people studied |
|---|---|---|---|---|---|
| Hahn 35 2007 | Neural networks | Full wave rectification and 5Hz low-pass filter | Vastus lateralis and biceps femoris | Isokinetic, eccentric, and concentric | 20 |
| Anwar et al31 2017 | Neural networks, fuzzy logic | Quadratic mean | Rectus femoris and vastus medialis | Isokinetic | 1 |
| Anwar &AI- Jumaily38 2017 | Support vector machine | Mean frequency, median frequency, total transformed spectral power, and wavelet | Rectus femoris, vastus medialis, vastus lateralis, biceps femoris, semitendinosus, semimembranosus | Isometric | 5 |
| Nurhanim et al.39 2017 | Particle swarm optimization | Quadratic mean | Vastus lateralis | Isokinetic | 1 |
| Peng et al.40 2015 | Neural networks | Full wave rectification and 2Hz low-pass filter | Rectus femoris, vastus lateralis, vastus medialis, biceps femoris, and semitendinosus | Eccentric and concentric | 1 |
| Menegaldo et al.41 2014 | Hill's muscle model | Rectification and bandpass filter | Rectus femoris, vastus medialis, and vastus lateralis | Isometric | 1 |
| Tsutsui et al.42 2005 | Neural networks | Rectification and moving average | Rectus femoris and biceps femoris | Isometric | 1 |
| Simon et al. 43 1995 | Polynomial model | Rectification and low-pass filter | Rectus femoris, vastus lateralis, vastus medialis, semitendinosus, and biceps femoris | Isokinetic | 5 |
| Heine et al.44 2018 | Hill's muscle model | Rectification and 6Hz low-pass filter | Vastus medialis, vastus lateralis, vastus medialis, and rectus femoris | Isokinetic | 1 |
| Ardestani et al.45 2014 | Wavelet neural networks | Quadratic mean and 1Hz low-pass filter | Semimembranosus, biceps femoris, vastus intermedius, vastus lateralis, and rectus femoris | Gait | 4 |
| Anwar & Anam45 2016 | Neural networks and machine learning | Mean frequency, median frequency, average power, total power, power spectral density, spectral momentum, and power spectral ratio | Rectus femoris, vastus medialis, vastus lateralis, biceps femoris, semitendinosus, semimembranosus | Isometric | 5 |
| Peng et al.47 2015 | Musculoskeletal model and optimization with genetic algorithms | 2Hz low-pass filter | Quadriceps, hamstrings, and gastrocnemius | Eccentric and concentric | 1 |
| Bai et al.48 2013 | Continuous wavelet transform | Mean frequency | Quadriceps and hamstrings | Eccentric and concentric | 10 |
| Simon et al.49 1994 | Pattern comparison | Rectification and low-pass filter | Rectus femoris, vastus lateralis, vastus medialis, biceps femoris, and semitendinosus | Isokinetic | 5 |
| Amarantini & Martin50 2004 | Optimization | Full wave rectification | Rectus femoris, vastus medialis, biceps femoris, and gastrocnemius | Site walks | 9 |
| Anwar & Al- Dmour51 2017 | Adaptive neural networks and fuzzy logic | - | Quadriceps | Isokinetic | 1 |
| Liu et al.52 2017 | Hill's muscle model | Full wave rectification, low-pass filter | Rectus femoris, vastus lateralis and semitendinosus | Eccentric and concentric | 1 |
| Shabani & Mahjoob 53 2016 | Hill's muscle model | Full wave rectification, 200Hz low pass filter | Rectus femoris, vastus medialis, vastus lateralis, semimembranosus, semitendinosus, and biceps femoris | Eccentric and concentric | 1 |
Source: Own elaboration.
Table 2 classifies the records included according to the year of publication. It shows that most articles were published in 2017, with 27.78%.
Table 2 Number of works included per year.
| Year | 1994 | 1995 | 2004 | 2005 | 2007 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Articles | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 5 | 1 |
Source: Own elaboration.
The Journal of Biomechanics was the source from (2 references). The remaining journals and conferences which the largest number of publications was retrieved only contributed one article each (Table 3).
Table 3 Sources of the publications included.
| Name of journal or conference | Number of articles | References |
|---|---|---|
| Journal of Biomechanics | 2 | 36,50 |
| Procedia Computer Science | 1 | 37 |
| 2016 International Conference on Systems in Medicine and Biology (ICSMB) | 1 | 38 |
| 2016 2nd IEEE International Symposium on Robotics and Manufacturing Automation (ROMA) | 1 | 39 |
| 2015 International Joint Conference on Neural Networks (IJCNN) | 1 | 40 |
| Biomedical engineering online | 1 | 41 |
| Optomechatronic Sensors and Instrumentation | 1 | 42 |
| Proceedings of 17th International Conference of the Engineering in Medicine and Biology Society | 1 | 43 |
| Medical Engineering & Physics | 1 | 44 |
| Expert Systems with Applications | 1 | 45 |
| 2016 6th IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob) | 1 | 46 |
| 2015 IEEE International Conference on Robotics and Biomimetics (ROBIO) | 1 | 47 |
| 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR) | 1 | 48 |
| Proceedings of 16th Annual International Conference of the IEEE Engineering in Medicine and Biology Society | 1 | 49 |
| 2017 IEEE Symposium Series on Computational Intelligence (SSCI) | 1 | 51 |
| 2017 IEEE International Conference on Cyborg and Bionic Systems (CBS) | 1 | 52 |
| 2016 4th International Conference on Robotics and Mechatronics (ICROM) | 1 | 53 |
Source: Own elaboration.
Of the 18 papers included, 14 used algorithms to calculate knee joint torque during the execution of motor tasks involving movement36,38-41,43,45,47-53 and 4 used them for motor tasks without joint movement.37,42,44,46
Each algorithm has different characteristics, such as the type of sEMG signal processing, the muscles used, the strategy implemented for the development of the algorithm, and the number of people studied. Some of the strategies used are neural networks, fuzzy logic, Hill's muscle model, support vector machines, particle swarm optimization, polynomial models, wavelet neural networks, and wavelet transform. Similarly, the algorithms differ in the types of contractions (concentric, eccentric, isokinetic, or isometric) used during sEMG signal detection.
Moreover, 13 of the articles reviewed used black-box techniques to estimate knee joint torque, while 5 did so using white-box models, specifically Hill's muscle models. Of the 13 investigations that opted for black-box models, 7 used neural networks; 3, regression and optimization-based models; 1, continuous wavelet transform; 1, vector support machines; and 1, pattern matching.
With this in mind, the authors of the present research describe below a work developed using neuronal networks, one using a regression model (black-box model), and another using a musculoskeletal model (white-box model).
First, Han36 estimated the knee joint torque of 20 individuals using a three-layer feed-forward artificial neural network in two stages. In the first stage, they were asked to perform the maximum voluntary contraction; in the second stage, they were asked to perform exercises at 30% and 60% within the whole range of motion of the knee, exercising eccentric and concentric contraction. In both stages, the measurements of the sEMG signals and joint torque were recorded. It should be noted that in the neural network model, the second layer contained a variable number of "hidden" units 5,10,15,20,25,30 that represented the portion of the network learning process in which most of the processing solution occurred. Also, age, sex, height, body mass, the envelopes of the sEMG signals of the agonist (vastus lateralis) and antagonist (biceps femoris) muscles, which were obtained from full wave rectification using a 5 Hz low-pass filter, the joint angle and joint speed were considered as predictive variables of net torque. The study concluded that artificial neural network models achieved a more accurate torque estimate (R=96) compared to stepwise regression models (R=0.76), that the accuracy of the model increased considerably when the number of "hidden" units increased from 5 to 10, that accuracy improved progressively as more hidden units were added, and that, according to the results obtained, it is possible to say that the performance of the model could be the best if 15 or more "hidden" units were used, achieving 100% convergence and 88% to 90% accuracy.
On the other hand, Simon et al.43 analyzed in 5 test subjects the relationship between the sEMG signals of the rectus femoris, vastus lateralis, vastus medialis, semitendinosus and biceps femoris muscles, as well as knee joint torque during flexion and extension. In this work, the authors designed a regression model as a function of angular position and velocity, the previous values of the torque and the rectified and smoothed sEMG signals. Based on this, they determined the coefficients using the least squares method from the information of 3 of the test subjects; the information of the 2 remaining subjects was used to validate the model. The authors obtained acceptable results in the validation subjects, where the RA2 values were 0.98 and 0.96 for extension, and 0.92 and 0.73 for flexion.
Finally, Peng et al.47 designed a model that consists of two main modules. Firstly, a muscle-tendon model calculates muscle force through the dynamics of muscle contraction; secondly, the values of these forces are entered into a musculoskeletal model to estimate joint torque. This model requires knowing details related to the muscles, such as length, force-length relationship, force-velocity relationship, among others; to validate it, the researchers used the mean squared error and the correlation coefficient, obtaining 3.65Nm in the first one and 0.96 points in the second one when they delayed the signal in 100ms. The results were considered logical due to the nature of the sEMG signal, which occurs 10-100ms before joint movement. It should be noted that this type of model allows us to know the individual contribution of each of the muscles studied, which can optimize patients' rehabilitation plans.
The algorithms of knee joint torque estimation found in this research have been developed by means of diverse techniques and their main objective is to estimate torque using the electrophysiological signals of the muscles of this joint. Unlike other algorithms that do not use muscle signals, they allow physical therapists to obtain additional and relevant information, such as muscle activation during rehabilitation processes.
Discussion
The processing of sEMG signals allows measuring knee joint torque during the execution of movements
According to the literature reviewed, there are multiple algorithms that allow estimating knee torque using sEMG signals from the muscles associated with the flexion and extension of this joint. 23% of the algorithms found are used for measurements under static conditions37,42,44,46 and the remaining 77% for measurements during the execution of movements.36,38,39-41,43,45,47-53 To develop these algorithms, techniques such as the Hill's muscle model,29,41,44 particle swarm optimization,39 polynomial models,49 wavelet neural networks and wavelet transform are used.45 Of these, only the Hill's muscle model is white-box because it is based on biomechanical models; the others are classified as black-box models since they do not pretend to know the structure of the study muscles.
Although there are methods based on biomechanical analyses and physical laws of motion dynamics to calculate the torque exerted by a subject during knee flexion and extension movements,54 algorithms based on electrophysiological signals, especially sEMG signals from the muscles of interest, are an effective alternative for measuring the torque exerted by this joint during movement and in different static positions.50 The latter method provides physical therapists with quantitative information to support the rehabilitation process of the subject since it allows assessing the activation and contraction of the muscles associated with the joint to be rehabilitated, in this case, the knee.9,28
Likewise, sEMG signals make it possible to objectively determine progress in terms of strengthening the muscles that provide stability to the knee joint. In practice, this is usually done by means of manual or external resistance elements, such as dumbbells, obtaining inaccurate measurements.
In this sense, estimating knee joint torque by means of sEMG signals has advantages as the measurement can be carried out with low-cost commercial devices, such as the MyoWare Muscle Sensor from Sparkfun Electronics. Similarly, these types of signals provide information related to the activation of the muscles involved in the joint of interest (knee) during exercises that require movement and resemble the muscles necessary for the development of activities of daily living. Finally, the algorithms for estimating joint torque based on black-box models 40,42,45,46 and using sEMG signals as input allow obtaining algorithms that behave appropriately for a specific subject without the need to know muscle parameters, which are required by Hill-type muscle models.
The sEMG signals have some limitations for the estimation of joint torque, such as the fact that the algorithms that focus on regressions and optimizations 39,43,50 seek to adjust the parameters of the models according to the experimental data obtained in a single person and, therefore, cannot be applied to any population. The same happens with algorithms based on neural networks: Anwar & Al-Jumaily38 did not validate it with data other than training data; Han36 trained a neural network to estimate joint torque in 20 people, but the training and the validation were done with information from a single patient, which can lead to an over-trained neural network; and Anwar & Al-Dmour51 trained a neuronal network with the data of a person for isokinetic exercises, with which acceptable results of torque estimation at low speeds were observed, however, the results for exercises at high speeds were not satisfactory and the information collected cannot be generalized.
On the other hand, Peng et al.40 & Bai et al.48 conducted studies in which they sought to provide an approximate measure of torque in the assessed joints by detecting user intent through sEMG signals. This approximate torque is used as input to rehabilitation systems for active-assisted exercises: however, it is not a precise torque. Finally, other studies were found41,44,47,52,53 in which algorithms based on the Hill's muscle model use information related to the muscles of interest, such as the length of the tendons, which varies according to the angle at which the joint is located. Nevertheless, this model requires the calibration of these parameters for each subject and the measurement of the maximum voluntary contraction in each session, which makes it a subject-dependent model.
It should be mentioned that, to measure knee joint torque and torque of any joint in general, the electrodes must be properly placed on the muscles of interest since the sEMG signal varies depending on that location. In addition, there are other variables that affect signal, such as crosstalk, skin impedance, sweating, and ambient and skin temperature.18
Most of the methods found require other signals besides sEMG signals to measure knee joint torque, such as kinematic signals36,37 and force signals.43 This implies that it is necessary to use additional elements to carry out the measurements.
Estimating knee torque using sEMG signals allows physical therapists to assess the condition of the muscles that provide stability to the joint and measure progress during rehabilitation
For decades, sEMGs have contributed to the diagnosis of various pathologies in the field of rehabilitation.19 According to the reviewed literature, the intensity of the sEMG signal is highly correlated with the intensity of muscle force, which allows estimating the intention of movement and joint torque.35-39 Moreover, some studies show that dynamic and static measurements, in different positions of the joint, allow determining the value of the maximum torque that the subject is able to exert.11,15,23,20
Technological advances to capture and extract information from sEMG signals make it possible to measure torque periodically. This provides the therapist with relevant information about the condition of the muscle and allows determining the progress of the subject during rehabilitation. In addition, the information obtained allows performing a quantitative evaluation of the patient's condition and, based on this, determining the adequate resistance that may be required to perform different motor tasks during the rehabilitation process of injuries to structures such as the anterior cruciate ligament11,17 and the menisci,16 as well as for gait training.25
Consistent with the above, sEMG signals could be used not only as an interface between humans and robotic rehabilitation systems, as is the case with exoskele-tons,36,40,41 but also as a strategy for patient assessment and joint torque measurement.
Physical therapists in Colombia do not usually have tools that allow them to obtain quantitative data to determine the patient's progress during the rehabilitation process.19,21 For this reason, the measurement of joint torque by means of sEMG signals would be of great help and would allow them to guide the intervention plan in accordance with clinical observations. However, it is necessary to determine the times and moments in which sEMG is used to quantitatively determine the state of the muscles that provide stability to the joint since muscle fatigue reduces the efficiency of the contractions and the movements performed,54 which could yield erroneous data on the progress of patients.
Exercises based on anisometric contractions and torque measurement during a sequence of joint movement allow determining patients' progress
Anisometric contractions are useful during therapeutic interventions because they allow increasing muscle force, power, and resistance by means of muscle fiber recruitment. This in turn optimizes joint stability and mobility and allows for a wide range of torque during a movement sequence, which can be estimated using algorithms that take sEMG signals as inputs.
During knee rehabilitation and training processes in athletes, it is important to determine the activity of the muscle during the execution of motor tasks to optimize the performance of the muscle based on the calculation of resistance and its influence in accessory muscles.19 According to this, sEMG signals are a tool that, in addition to estimating joint torque, allows monitoring the electrical activity of the muscles.
In this scenario, it is proposed that measuring joint torque by means of sEMG signals is of great help for physical therapists during the diagnostic phase since they allow defining the therapeutic objectives based on quantitative data, determining the capacity of muscle fiber recruitment during the execution of the movement, establishing the appropriate resistance for the execution of motor tasks, and determining the progress of the patients during the rehabilitation process.50
Conclusions
The present literature review led to find an important number of publications that document the calculation of knee joint torque from sEMG signals during the execution of anisometric exercises. However, no publications were identified in which the torque calculated from sEMG signals was used in rehabilitation processes as such, so it is necessary to carry out research on this topic, which promises interesting applications in physical therapy.
Results regarding the measurement of knee joint torque from sEMG signals are an application of the biomedical signal processing theory and, therefore, an alternative route to traditional work in biomechanics and rehabilitation, which usually involves the application of mechanical laws.
In practice, measuring joint torque dynamically using sEMG signals represents an easily accessible and low-cost alternative to the use of isokinetic dynamometers for the patient's rehabilitation process. This alternative is also an option that expands the possibilities of monitoring and assessment.
Another advantage of measuring knee joint torque using sEMG signals is that they are always available for processing and, therefore, the physical therapist permanently has data on muscle activation, which are not provided by other joint torque measurement technologies. However, sEMG signals also have limitations because they require professionals to have basic knowledge of the capture technique to obtain good-quality results.

