











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The Hall Technique was first described in 2006 by Innes NPT et al, as a method for treating primary molars affected by caries, using preformed steel crowns without the need for local anesthesia, caries removal, or tooth preparation 1. Background and illustration of the original technique has been reported 2,3 and since then, different randomized clinical studies have shown long-term success of up to 92% at 5 years 4, values hardly achieved with any another restorative treatment.
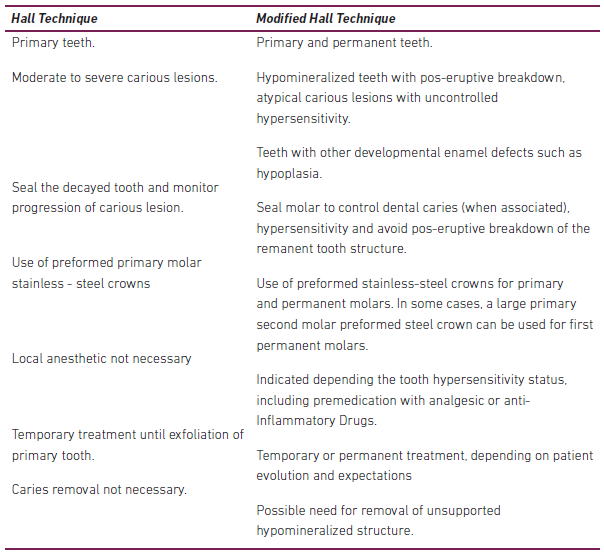
Treatment of molars affected by severe Molar Incisor Hypomineralization (MIH) and deciduous molar hypomineralization (DMH) is a challenge for the clinician, given that structural alterations and tooth composition affect the performance of adhesive materials 5. In this context, a Modified Hall Technique could be a successful and easily applied alternative for the management of hypomineralized molars (Table 1).
Description of the cases
The case reports that are presented below, are based on the Case Report guidelines (CARE).
Case 1
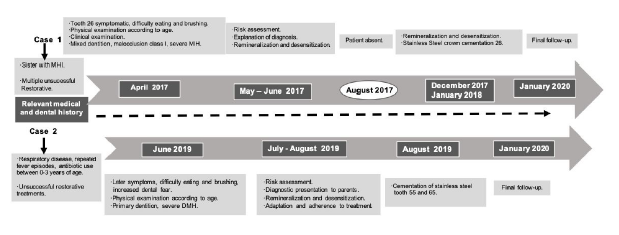
Ten-year old female patient who consulted CES University Pediatric Dental Clinics in April 2017 (Figure 1); chief complaint was pain in the upper left first permanent molar region. The patient presented sensitivity to air, hot and cold foods and drinks, and difficulty performing adequate oral hygiene. Upon clinical examination, the upper left first permanent molar as well the upper central incisors revealed opacities and loss of tooth structure characteristic of severe MIH (Figures 2a-2b). A preformed stainless-steel crown (E-UL#7 - 3M® ESPE crown, New York, USA) using the Modified Hall Technique was cemented on the upper left first permanent molar (Figures 2b-2c-2d).
Case 2
Five-year-old female patient who consulted CES University Pediatric Dental Clinics in August 2019 (Figure 1). Parents reported a history of restorative treatments of primary second molars, and pain caused by hot and cold foods and drinks as well during tooth brushing. On clinical examination, the upper second primary right molar presented opacity with loss of tooth structure and a composite restoration; the upper second left primary molar presented atypical restorations, characteristic of severe DMH (Figure 3a-3b-3c). In addition, patient presented increased dental fear and anxiety. Treatment included placement of preformed stainless-steel crowns (E - UR # 5 and E-UL # 5 - 3M® ESPE, New York, USA) on the affected molars, using the Modified Hall Technique (Figures 3a-3c-3d).
Description of Modified Hall Technique
In the two cases presented an initial measurement and selection of a prefabricated steel crown for each tooth was made; afterwards, an interproximal spacer was installed for one week (Figure 2b-3a-3c). At a second appointment, the elastic was removed, and the patient was anesthetized with topical anesthesia (Garhocaína®, Bogotá, Colombia) and lidocaine with epinephrine (New Stetic®, Guarne, Colombia) using an infiltration technique. The crown was then measured, adapted and removed and finally teeth were washed and dried. Crown cementation was done with relative isolation, digital pressure, and type I glass ionomer cement (Ketac Molar Easymix, 3M® ESPE, New York, USA) (Figures 2c-3d). Patients were asked to bite down on a cotton roll to finish setting the crown. Excess material was removed, and a dental floss was passed between the proximal surfaces. Immediately after cementation there was an initial increase in vertical overbite. In case 1, overbite decreased from an initial 30% (Figure 2d) to 10% (Figure 2f). In case 2, it varied from an initial 15% (Figure 3e) to an open bite (Figure 3f). One-month follow-up showed that overbite reversed to initial measurements in both patients, and no changes were detected in soft, hard and support tissues (Figure 2e- 3d).
Preventive professional measures were implemented in both patients in order to prevent dental caries including diet counseling, use of fluoride toothpaste with 1,450 ppm, plaque control, and monthly professional follow-up examinations accompanied with prophylaxis and topical application of 1,23% acidulated during a 6-month period.

Figure 2 Severe MIH clinical examination - modified Hall technical steel crown installation and two-year follow-up. 2a. Tooth 11 exhibits a cream, yellow and brown opacity with structural tooth loss; Tooth 21 presents well demarcated white opacity. 2b. Modified Hall Technique on 26; adaptation of elastic between tooth 65 and 26; 2c. Stainless Steel Crown cemented on 26. 2d. Occlusion after cementation. 2e-2f. Two-year follow-up of Severe MIH case. 2e. Crown on tooth 26 is well adapted and periodontal and dental integrity are evident. 2f. Permanent dentition with stable occlusion.

Figure 3 DMH severe clinical examination - Hall technical steel crown installation modified and 6-month follow-up. 3a. Tooth 55 presents fractured restoration, brown opacity, and structural loss on the palatal surface; elastic between teeth 55 and 54. 3b Initial occlusion. 3c. Tooth 65 with fractured and dislodged restorative material on occlusal and palatal surfaces. Elastic between teeth 64 and 65. 3d. Stainless steel crown on tooth 55 immediately after cementation. 3e. Occlusion after cementation. 3f. Occlusion at six-month follow-up.
Discussion
MIH/DMH is an increasingly frequent condition observed in clinical practice 6-8. The treatment of severely affected molars can vary from temporary glass ionomer cement restorations to tooth extraction 9. Although adhesive techniques and materials can also be used, ultra-structural alteration and composition of these teeth can compromise clinical performance of said restorations 10.
In a case report published by Quintero et al 11 , the authors proposed the “Hall technique” for the treatment of severely hypomineralized molars which was ori-ginally described for treatment of primary molars with dental caries lesions. Given the above, we propose that in cases with MIH/DMH and other developmental enamel defects (DED), the term “Modified Hall Technique” be used. For example, a preformed steel crown for a primary tooth may be placed on a permanent first molar with severe MIH that requires use of local anesthesia due to the hypersensitivity that patients experience 12, as reported in case 1.
An advantage of the Modified Hall Technique, is that it can be used in patients with a history of negative dental experience, fear and dental anxiety, which is frequently reported in these patients 13; this, given that it is a fast and non-invasive procedure that does not require tooth preparation. These behavioral characteristics are frequently found in the MIH patient, as reported by Jälevik and Klingberg in 2002, who found that patients affected by MIH had higher levels of dental fear and anxiety 13. This information is valuable to select non-invasive and comfortable options for the patient when designing the treatment plan.
Another advantage refers to its long-term success rate as reported by Innes et al, who found a success rate of 92% at five years compared to 52% in a control group with conventional restorative treatment 4. Moreover, despite being a metallic restoration and not considered to be esthetic, studies also indicate that it is well accepted by parents and patients 14.
One concern that may exist when placing crowns with Modified Hall Technique is the increased vertical dimension of the patient’s occlusion. In the reported cases, an increased vertical dimension was observed immediately after cementation, but it returned to its normal dimension one month later in both patients. There are limited studies that have evaluated the effect of this technique 14; only one study, evaluated and found that it had no effect on the temporomandibular joint (TMJ) in children between 5 and 9 years of age 15. This shows the need for future long-term clinical studies that evaluate the changes in vertical dimension or the TMJ in patients treated with either the Hall Technique or the Modified Hall Technique.
A limitation of steel crowns is the accumulation of dental plaque and gingival inflammation. Therefore, it is important that the clinician verify the adaptation of the crown immediately after cementation and carry out periodic clinical and/or radiographic controls according to the risk level of the patient. Likewise, individual and professional control strategies for dental caries should be adopted.
Finally, it is important to emphasize the importance of making an early diagnosis of enamel developmental defects, that allows less invasive and uncomfortable treatments for the patient and improvement of long-term prognosis.

