










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957
Rev Col Gastroenterol vol.35 no.1 Bogotá ene./mar. 2020
https://doi.org/10.22516/25007440.324
Case report
Post-colonoscopy appendicitis: Case report and literature review
1Médico cirujano, epidemiólogo, residente de cirugía general. Universidad del Rosario y Hospital Universitario Mayor. Bogotá, Colombia
2Médico cirujano, residente de cirugía general. Universidad del Rosario y Hospital Universitario Mayor. Bogotá, Colombia
3Médico cirujano, Fellowship en Coloproctología. Universidad del Rosario y Hospital Universitario Mayor. Hospital Universitario Barrios Unidos. Bogotá, Colombia
4Médico cirujano, coloproctólogo. Jefe del servicio de coloproctología del Hospital Universitario Mayor - Méderi. Bogotá, Colombia
We present the case of an 83-year-old patient who had no significant medical history. A screening colonoscopy had been performed three 3 hours before onset of pain in the right iliac fossa. Twelve hours later, the patient to the emergency department. Physicians suspected that the pain was a complication related to colonoscopy and ordered an abdominal CT scan which showed tomographic signs of appendicitis. A laparoscopic appendectomy was performed and removed a perforated cecal appendix without complications.
Keywords: Colonoscopy; appendicitis; complication
Presentamos el caso de una paciente de 83 años sin antecedentes de importancia, a quien se le realizó una colonoscopia de tamización 3 h antes del inicio de la sintomatología. La paciente consultó al servicio de urgencias por presentar dolor en la fosa ilíaca derecha de 12 h de evolución. En efecto, durante el examen físico, se encontró un dolor localizado en la fosa ilíaca derecha.
Ante la sospecha de una complicación relacionada con la colonoscopia, se ordenó una tomografía de abdomen, la cual mostró signos tomográficos de apendicitis. Se realizó entonces una apendicetomía por laparoscopia, sin complicaciones, pero se evidenció un apéndice cecal perforado.
Palabras clave: Colonoscopia; apendicitis; complicación
Introduction
In medical practice, a complication is the unfavorable result of a diagnostic or therapeutic procedure. While an intervention is performed in order to obtain a benefit, it can cause damage. Therefore, before carrying out a procedure, we must always calculate the probability of complications and balance that against the possible benefits. 1
Colonoscopies are routinely performed in coloproctology and gastroenterology services around the world. They are the procedure of choice for screening for colorectal cancer and are used for the diagnosis and treatment of other pathologies of the colorectal mucosa.
Nevertheless, they are not harmless: complications include perforations, bleeding and damage to the spleen. Less frequent complications include priapism, intestinal obstructions, mesenteric ischemia, cecal volvulus, pancreatitis, perforations of the small intestine and appendicitis. 1
Appendicitis following colonoscopy is a very rare complication whose reported incidence is approximately 0.038%. Its incidence is difficult to establish since there are only case reports: until 2017 only 41 cases had been described and only one of these was in Latin America. 2,3
Clinical case
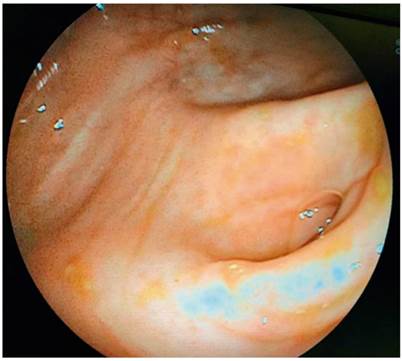
Our patient is an 83-year-old woman who had no pathological history of interest. She underwent diagnostic colonoscopy which found multiple diverticula in the sigmoid colon. The complete examination lasted approximately 12 minutes. No alterations were found in the cecum, the appendicular orifice, nor the rest of the colon (Figure 1). The patient was discharged without any evidence of any complications.
Twelve hours after the procedure, the patient came to the emergency department because of increasingly intense abdominal pain, located in the right iliac fossa. The pain had begun three hours after discharge. During physical examination, pain located in the right iliac fossa with abdominal guarding was striking.
Paraclinical tests found leukocytosis (20.6 x 109 Cel/L) and neutrophilia (90%). An abdominal CT scan, performed because of suspicion of perforation due to the colonoscopy (Figure 2), found an 11-mm retrocecal appendix with alteration of the adjacent fat. A laparoscopic appendectomy was then performed.

The surgical procedure, carried out without complications, found a perforated cecal appendix with a small amount of peritoneal reaction fluid in the right iliac fossa. The postoperative period was without complications, and the patient was discharge three days after the procedure. The pathology study confirmed acute perforated appendicitis and periappendicitis.
Discussion
Acute appendicitis following colonoscopy is rare. It was first described in 1988 by Houghton and Aston, 4 but since then 41 additional cases have been reported. Only one of them is from Latin America. This is a difficult diagnosis to make since the pain may be secondary to retained gas or a colonic spasm secondary to colonoscopy.
Post-colonoscopy acute appendicitis should be differentiated from post-polypectomy syndrome which presents with a similar symptoms of pain, peritoneal irritation, leukocytosis, and fever. 3
Of the cases reported in the literature, the majority are men, and the median age is 53.9 years. The oldest patient reported was 84 years old. Time between colonoscopy and appearance of symptoms varies, but in 28 cases, onset of pain occurred during the first 24 hours, as was the case above.
Among the cases analyzed, four received conservative treatment and treatment was not specified in five cases. The rest of the patients were treated surgically as in our patient’s case. Among the intraoperative findings, there were 14 perforated appendixes (as in our patient). 5,6 This may be related to the mechanism of injury during colonoscopy. 7
An abdominal CT scan is the study of choice for preoperative diagnosis because the pain may have non-surgical origins or may be related to more frequent complications. An abdominal CT scan’s findings helps establish definitive management.
Theories about the causes of acute post-colonoscopy appendicitis include those related to subclinical pathology of the appendix, barotrauma, fecal impaction, intubation of the appendicular lumen, and damage of the mucosa around the appendicular orifice. 3,8
While development of post-colonoscopy appendicitis might be considered coincidental, perhaps Ockham’s razor suggests that there is indeed a causal relationship. Since this question has not been fully elucidated, 9 the question arises: coincidence or causality?
Conclusions
Post-colonoscopy appendicitis is a rare complication whose true incidence remains unknown since the number of cases reported is very small worldwide. However, this condition should always be included in the differential diagnosis of patients with abdominal pain after colonoscopy. Timely diagnosis is the cornerstone for avoidance of complications.
Referencias
1. Church J. Complications of colonoscopy. Gastroenterol Clin North Am. 2013;42(3):639-57. http://dx.doi.org/10.1016/j.gtc.2013.05.003 [ Links ]
2. Loureiro M, Bonin E, Leiner C, Weigmann SC, Fontana A. Apendicite aguda pós colonoscopia: desafio diagnóstico e tratamento minimamente invasivo - relato de caso. Rev Col Bras Cir. 2011;38(5):365-368. https://doi.org/10.1590/S0100-69912011000500015 [ Links ]
3. Chae HS, Jeon SY, Nam WS, Kim HK, Kim JS, Kim JS, et al. Acute appendicitis caused by colonoscopy. Korean J Intern Med. 2007;22(4):308-311. https://doi.org/10.3904/kjim.2007.22.4.308 [ Links ]
4. Houghton A, Aston N. Appendicitis complicating colonoscopy. Gastrointest Endosc. 1988;34(6):489. https://doi.org/10.1016/S0016-5107(88)71451-0 [ Links ]
5. Paramythiotis D, Kofina K, Papadopoulos V, Michalopoulos A. Diagnostic Colonoscopy Leading to Perforated Appendicitis: A Case Report and Systematic Literature Review. Case Rep Gastrointest Med. 2016;2016:1378046. https://doi.org/10.1155/2016/1378046 [ Links ]
6. Sanz M, Labarta M, Cuartero B, Mejía D. Apendicitis: complicación de una colonoscopia. Hospi Clínico Univ Miguel Servet. 2011:2-6. [ Links ]
7. Zhou XC, Huang CW, Dai YY, Huang ZY, Lou Z. Perforated appendicitis after colonoscopy: cause or coincidence? A rare case report and literature review. Medicine (Baltimore). 2017;96(46):e8747. https://doi.org/10.1097/MD.0000000000008747 [ Links ]
8. Rodríguez-Otero Luppi C, Salas Muñoz J, Targarona EM, Rodríguez Blanco M, Bollo J, Trias M. Acute appendicitis after colonoscopy: coincidence or cause? Gastroenterol Hepatol. 2011;34(7):516-7. https://doi.org/10.1016/j.gastrohep.2011.04.004 [ Links ]
9. Shaw D, Gallardo G, Basson MD. Post-colonoscopy appendicitis: A case report and systematic review. World J Gastrointest Surg. 2013;5(10):259-263. https://doi.org/10.4240/wjgs.v5.i10.259 [ Links ]
Received: December 03, 2018; Accepted: January 20, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
