











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Worldwide, ischemic stroke is the primary cause of long-term disability among adults between 45 to 65 years1. One-third of ischemic stroke patients are functionally dependent in the following three to six months after ischemic stroke, leading to work withdrawal, difficulty in social participation, and inferior Health-Related Quality of Life (HRQoL)2. HRQoL measuring tools include the short Form 36 (SF-36), EuroQOL (EQ-5D), Sickness Impact Profile (SIP), Stroke-Specific Quality of Life Scale (SS-QOL) and the Stroke Impact Scale (SIS), to mention some3. The advantage of some scales is their high accuracy on the most affected domains affected in stroke-survivors3. Post-stroke disability domain is commonly assessed by the modified Rankin Scale (mRS). However, mRS could poorly represent the real impact of quality of life in stroke2,3. For instance, patients with visual or communication impairment but otherwise independent in activities of daily living punctuated mRS 0 or 1, which is considered a favorable clinical outcome4-7.
Stroke impacts different aspects of life, such as psychological, social, and economic spheres of the patients, their families, and in general society8,9. The stroke impact is particularly relevant for healthcare providers and researchers, to whom HRQoL approaches rely on patient-reported outcomes (PROs) to evaluate care and the result8,9. Measures that assess HRQoL, such as the EuroQol 5-dimension questionnaire, reflect the importance of some aspects that reduce the quality of life, which escape from the mRS measurement and might be significantly relevant to patients and as a tool to focus further rehabilitation efforts8,9.
Since HRQoL is a multidimensional concept, a combination between EQ-5D and mRS might help to overcome limitations such as the ceiling effect and improve discriminatory power10. Previous studies have demonstrated a poor correlation with the EQ-5D visual analog scale (EQ-5D VAS) and mRS10. As it is known, patients with disability (mRS ≥ 3) have poor QOL; however, those aspects are not assessed by mRS alone. We aim to assess HRQoL evidence, applying EQ-5D in Colombian patients with ischemic stroke and correlating its results with the mRS.
Methods
Analytical cross-sectional study in a cohort of ischemic stroke patients in Colombia. We included 91 patients who were hospitalized at Hospital Internacional de Colombia, Fundación Cardiovascular de Colombia, and Clínica Bucaramanga from December 2015 to July 2017 due to a first or a second acute ischemic stroke, and seen again at three months as a median follow-up (Q1: 1- Q3:3) after their event. Patients aged > 18 years, no sex predilection, who were evaluated by a neurologist during the acute stroke period were included in the study. All of the patients who died during the whole follow-up after stroke and whose available information was inadequate were excluded in the study.
At baseline, data were collected from medical records such as level of education, National Institutes of Health Stroke Scale (NIHSS) score on admission, pre-stroke disability using the mRS. Comorbidities like hypertension, prior stroke, diabetes mellitus, cardiac disease, chronic obstructive pulmonary disease and renal impairment were defined by documented history and active medications or clinical or laboratory findings at presentation.
Questionnaires at 6 to 12 months post-discharge were performed via telephone by trained physician interviewers at the coordinating center. Re-hospitalization, working, marital status, and pre-stroke disability were measured using the mRS and HRQoL.
Patient-Reported Outcome Measures
HRQoL was assessed with the EQ-5D questionnaire, which has been validated in stroke10 and has the advantage of its simplicity and accessibility to the patient11. In patients with aphasia, the questionnaire was collected from their caregivers. EQ-5D comprises of two parts: first, a short descriptive health status with five domains (Mobility, Selfcare, Usual activities, Pain/Discomfort, and Anxiety/Depression), each domain has five severity responses levels (none, slight, moderate, severe, and unable to/extreme). The EQ-5D state of health can be summarized using a 5-digit code or an index value. The EuroQol -creator of the questionnaire- disposed of crosswalk value sets (the index values for all possible EQ-5D health states) available on their website. We used the value set described in Spain, in which state 55555 means severely affected in all five dimensions and an index value - 0.654, whereas state 11111 means not affected in any of the dimensions and an index value 1 (best possible health). A total of 3125 possible health states are defined in this way for EQ-5D-5L. Second, the EQ-5D VAS provides a quantitative measure of the patient's perception of their overall health. The EQ-5D VAS is numbered from 0 (the worst health you can imagine) to 100 (the best health you can imagine)11.
Clinician-Reported Measures
We measured the NIHSS, pre and post-stroke mRS, and the Charlson comorbidity index.
The NIHSS is a stroke scale that measures neurological deficits, contains 15 evaluated items with scores ranging from 0 to 42 where higher scores indicate more significant impairment12.
The mRS assesses disability and dependence for daily activities after stroke. The mRS scores range from 0 to 6, meaning grade 0 (no residual symptoms), grade 1 (no significant disability), grade 2 (slight disability), grade 3 (moderate disability), grade 4 (moderately severe disability), grade 5 (severe disability) and grade 6 (the patient has expired)13.
The Charlson comorbidity index classifies 17 relevant comorbidities and predicts the risk of death in the following year14.
Data analysis
Descriptive statistics data are expressed as a number (percent), mean (SD), or median (interquartile range) as appropriate. Prespecified variables included post-stroke disability by mRS (no disability ≤ 2 vs. disability ≥3), EQ-5D domains scores (without impaired 1-2 vs. with impaired 3-5). We assessed for differences in baseline demographic, NIHSS, Charlson comorbidity index, variables among those with and without disability at 3 months as median follow-up (Q1: 1- Q3:3) after their event using the T student test for independent variables, Pearson X2 tests for categorical variables, and MannWhitney U tests for categorical variables, ordinal variables, and non-parametric distributed continuous variables.
We used Spearman correlation coefficients (rs) to assess the association between measures because EQ-5D, EQ-5D VAS, and mRS are ordinal variables. We also performed the Exact McNemar test to compare mRS proportions before and after stroke.
Independent robust simple linear regression models were performed (because there was no normal distribution of the outcome variable) using the VAS as an outcome and as possible predictors the dimensions of the HRQoL and the modified Rankin both in its original scale and in its dichotomous form. Statistical significance was considered to be p value < 0.05 and all tests were performed on two tails. The statistical analysis was performed using Stata version 14.0
Ethical considerations: Our study complies with the ethical standards of the Declarations of Helsinki. The institutional review board approved this study from each institution prior to its initiation. The patients or caregivers gave written informed consent to participate in this study.
Results
Population
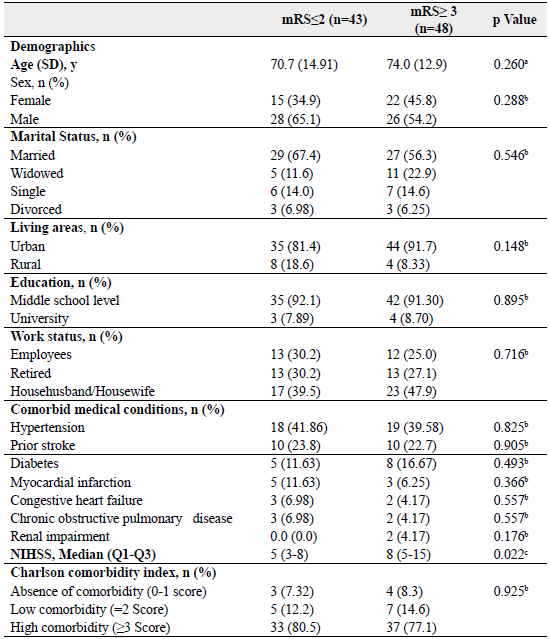
Among 91 patients, the mean age was 71.2 (SD 13.9); 59.3% (54) were male and 10% (9) underwent thrombolytic therapy. To analyze our population, we stratified by post-stroke mRS ≤2 and ≥3. At the acute ischemic stroke admission, the median NIHSS score was 5 (Q1: 3 - Q3:8) in patients with mRS ≤2 and 8 (Q1: 5 - Q3:15) in patients with mRS ≥3 (p = 0.022). There was no significant difference in baseline demographics, prior stroke, and the Charlson comorbidity index in our population by mRS, Table 1. The majority of patients were independent (mRS ≤2) before stroke (90%). After stroke, about half were (47%) (p < 0.001).
Patient-Reported Outcome Measures
Figure 1 shows the median EQ-5D index value was 0.63 (Q1:1.0 - Q3:0.26). The best possible health status (state 11111) was achieved in 26.9% of the population, while the rest of the population had at least one affected domain, all with global statistically significant differences by mRS (p=0.021). Assessment of the individual domains of the EQ-5D showed that the domain most affected was usual activities (59.5%), but in general, more than 60% of the population was affected in at least one of any of the five domains.
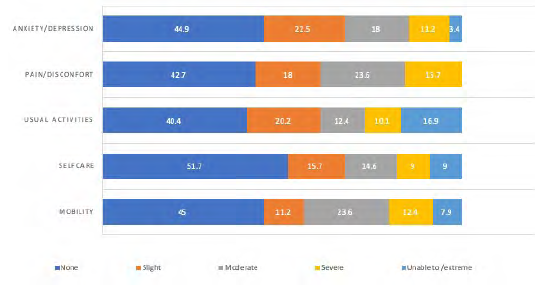
Figure 1 EQ-5D impaired domains of the Colombian patients, 2015 and 2017 Source: Based on results obtained from the analysis of our study.
We found statistically significant differences between post-stroke mRS (≤ 2 vs ≥ 3) in each EQ-5D domains: mobility (p<0.001), usual activities (p<0.001), self-care (p<0.001), anxiety/depression (p<0.001) and pain/discomfort (p<0.001). Figure 2 shows the median EQ-5D VAS in patients with mRS < 2 was 90 (Q1:80 - Q3:90), and in patients with mRS > 3, the median was 60 (Q1:50 - Q3:80) (p<0.001).
Correlations between EQ-5D VAS and all EQ-5D domains were inverse, negative and moderate with the highest for mobility (rs -0.69, p<0.001) and the lowest for pain/discomfort (rs -0.52, p<0.001). Patients experiencing effects in any EQ-5D domain had significantly lower EQ-5D VAS (Figure 1). The Table 2 shows correlation between EQ-5D VAS and EQ-5D index was rs 0.66 and between EQ-5D VAS and mRS was rs -0.58 (p<0.001).
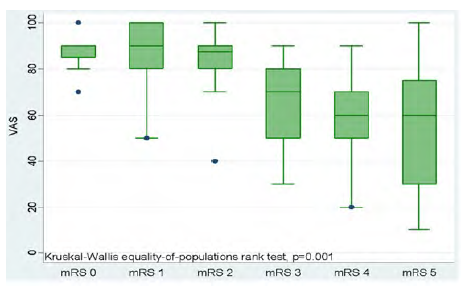
Figure 2 Distribution of mean EQ-5D VAS across mRS scores, Colombia, 2015 and 2017 Source: Based on results obtained from the analysis of our study.
Table 2 Correlation among EQ-5D VAS and EQ-5D affected domains, and the Proportion of Variation in EQ-5D VAS by the EQ-5D and disability. Colombia, 2015 and 2017
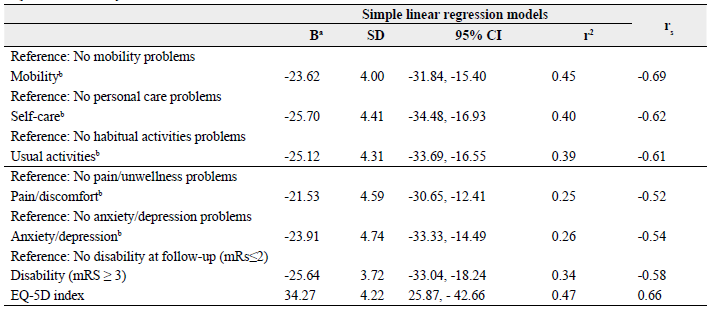
Source: Based on results obtained from the analysis of our Study. a Indicate the mean difference in EQ-5D VAS score between patients with affected domains in the EQ-5D scores compared with the patients without. b Not affected results in 1-2 severity response levels and affected domains 3-5 respectively.
rs = Spearman correlation coefficients
r2 = calculated from robust simple regression model for the dichotomous type variable.
Simple linear regression model
We found that the variation of EQ-5D VAS score (dependent variable) is explained in 47% of cases by the EQ-5D index (independent variable), Table 2. Patients with self-care difficulties reduce their perception on EQ-5D VAS score by 25.70 points, trouble participating in usual activities by 25.12 points, experiencing anxiety/ depression by 23.91 points, issues with mobility by 23.62 and the presence of pain/discomfort by 21.53 points in comparison with patients who did not experience negative effects. Table 2 shows that patients with a disability (mRS ≥ 3) had lower levels of QOL based on EQ-5D VAS score than patients with complications in the EQ-5D domains. These participants with mRS ≥ 3 reduced their EQ-5D VAS score by 25.64 points, almost the same reduction caused by a complication in just one domain like self-care (-25.70). However, when analyzing the change in EQ-5D VAS score, we observed that patients with difficulty in mobility (45%), self-care (40%) and usual activities domains (39%), independently explained higher variability in EQ-5D VAS scores than patients with mRS ≥ 3 (34%).
Discussion
The correlation between EQ-5D and mRS was found as it is established15. Among patients with a disability (mRS ≥ 3), a notable proportion had significant complications in EQ-5D domains, poor HRQoL due to stroke. Our findings support previous studies that report that the mRS might fail to capture some outcomes in ischemic stroke patients beyond motor disability11.
The EQ-5D results showed significant predictors of ischemic stroke outcomes (such as pain/discomfort and anxiety/depression). We found that the mRS correlated more with motor domains (such as mobility, self-care, and usual activities). One contributing factor to these findings is that mRS has a strong correlation with domains representing motor function with only a modest correlation with the rest of EQ-5D domains11. We demonstrated in this analysis that EQ-5D could show both psychological and physical impairments that are important for stroke patients even if those have a minimal residual disability after stroke11.
The VAS was the focus of additional analysis with mRS because it had one of the lowest variabilities with mRS compared with the EQ index. Also, based on our findings, the EQ-5D VAS global score reduced significantly in patients with mRS ≥3. One explanation is that patients who have an excellent functional outcome and suffer little from psychosocial aspects might have better HRQoL; variables such as optimism, self-esteem, perceived control, and social support play an essential role, but those were not assessed in this study16. Interestingly, we found that the average VAS in this study was 80, better than in previous studies on ischemic stroke survivors14.
HRQoL is a parameter that interferes with the definition of treatment as a primary point of rehabilitation. EQ-5D results provide context regarding the reasons for disability (e.g., trouble with mobility, inability to manage themselves)16. EQ-5D might overcome ceiling effects known to limit the mRS, as referred to in previous reports16. Numerous studies in ischemic stroke patients without disability (mRS ≤ 2) reported that the same patients had a reduction in arm use, which might be a shortcoming of the mRS scoring16. These findings can show substantial interobserver variability rather than true patient status due to disability, especially from the patient's perspective16.
Our study has several significant strengths. First, to our knowledge, this is the first study of EQ-5D only in ischemic stroke patients from a population in Colombia and data collected longitudinally17. Other studies have validated it by looking at chronic diseases in the general population18. In Latin America, there are only a few reports in countries, like Brazil, where the validity and reliability of the EQ-5D were evaluated in stroke patients with unilateral spatial neglect19. The American Heart Association included the use of PROs in both clinical practice and research, knowing that the patient's perspective allows more informed treatment decisions and can improve recognition of these potential complications20. Second, the cross-sectional study was from three institutions that had patients with different severities of ischemic stroke, resulting in broad results for PROs and mRS scores, which in chronic diseases such as stroke, with sequelae that are sometimes incurable or insufficiently understood, a realistic goal of healthcare providers is to improve functional status or quality of life. These can only be accurately self-reported by survivors21.
There are also limitations in this study. First, we only interviewed patients once (at 6 or 12 months), which made our results impossible to transpose; we did not evaluate over time to determine worsening or improvement in HRQoL related to other medical conditions. However, it is recognized that most of the improvement in stroke patients occurs in the first 90 days to one year. Our evaluation was performed in an appropriate period22. Second, we did not include other domains that might be affected by stroke, such as cognition, specific emotional consequences, family dynamics, social support, and sleep disorders12. Third, severely impaired patients received help to complete EQ-5D-5L questionnaires from their caregiver because they had communication or cognitive impairments, reducing the validity of these responses in some domains such as those involving psychosocial states23. Fourth, we relied on the EQ-5D-5L Spain value because, at the moment, there is not a value set for Colombia.
Stroke survivors cope well after the acute event, mainly because of reperfusion therapies and rehabilitation24. The health domain representing physical function (usual activities) was the most frequently affected, consistent with the results of previous reports25. Notably, in our results, a very relative proportion of patients also report complaints in the pain/discomfort dimension, which is identified in only 2.7% of stroke cases26. The reasons for the pain/discomfort dimension were not ascertained but could be attributable to the bi-directional relationship between anxiety or depression and pain27. Pain and emotional consequences after stroke are missed, leading to inadequate treatment or no treatment28.
Further studies will explain more of these findings and the necessity of screening for these conditions that patients might benefit from the treatment of. The EQ-5D instrument is straightforward to apply, considering dimensions that mRS does not access. Although mRS is one of the most commonly used disability measures in stroke, it focuses primarily on motor functions that might reduce its utility in assessing the global health status of patients with stroke29.
Importantly, consequences after stroke could be related as well as non-related to it, such as spasticity, frozen/stiff joints or depression, but other complaints could be attributable to age-related changes, such as fatigue, arthritis, or muscle soreness29. These kinds of consequences could be attributable to comorbidities, such as diabetes and renal impairment, as demonstrated in this analysis in patients with mRS ≥3.
Conclusion
The EQ-5D provides additional information in stroke patients unmeasured in the traditional clinical-reported disability scale (mRS). Although EQ-5D and mRS evaluated different spheres on stroke patients, applying the EQ-5D instrument in real-world clinical settings might contribute multidimensional information on how life is affected after a stroke. This kind of information might be useful to plan further studies and provision of services in stroke survivors.

