










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
versión impresa ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.23 no.2 Medellín ene./jun. 2012
ORIGINAL ARTICLES DERIVED FROM RESEARCH
Clinical and radiographic comparison of the pendulum effect with skeletal anchorage versus dentoalveolar anchorage1
Sandra Liliana Gómez Gómez2; John Jairo Betancur Pérez3; Jorge Alberto Arismendi4; Jorge Humberto Gil Cardona5
1 Article derived from a research project carried out as partial requirement
to opt to the title of Specialist in Orthodontics, at the School of Dentistry,
by one of the co-authors
2 Dentist. Specialist in Teenager Comprehensive Dentistry and
Orthodontics, Assistant Professor, School of Dentistry, Universidad
de Antioquia, Medellín, Colombia. Email address: sandraligomez@une.net.co
3 Dentist. Specialist in Teenager Comprehensive Dentistry and
Orthodontics; Specialist in Health Services Administration: Marketing;
Specialist in Higher Education. Assistant Professor, School of Dentistry,
Universidad de Antioquia, Medellín, Colombia. Email address: acelba@une.net.co
4 Dentist. Specialist in Adult Comprehensive Dentistry, School of
Dentistry, Universidad de Antioquia. Associate Professor, Vice-Dean,
School of Dentistry, Universidad de Antioquia. Medellín, Colombia.
Email address: jorgearismendi@une.net.co
5 Dentist. Specialist in Teenager Comprehensive Dentistry and
Orthodontics, School of Dentistry, Universidad de Antioquia. Medellín,
Colombia. Email address: jorgehumbertogil@hotmail.com
SUBMITTED: JUNE 7/2011 16/2011 - ACCEPTED: FEBRUARY 28/2011
Durán AK, Lucumí ÁC, Zapata LM, Correa H, Garzón H. Effects of LED/laser on the enamel due to exposure during dental bleaching. Rev Fac Odontol Univ Antioq 2012; 23(2): 256-267.
ABSTRACT
INTRODUCTION: This study seeks to clinically and radiographically compare the effects produced by the distalization pendulum
in both skeletal and dentoalveolar anchorage, in patients with Class II malocclusions at the Universidad de Antioquia's School of Dentistry
METHODS: a pre-experimental comparative study was carried out on a sample of 19 patients aged 15-26 years, divided into two groups:
9 patients treated with bone anchorage pendulum and 10 with dentoalveolar anchorage pendulum. Lateral cephalic radiographs of each
patient were taken and study models were done at the beginning and the end of evaluation period (6 months).
RESULTS: both clinical and
radiographic results show significant differences in the effects produced at the incisors and molars. The pendulum with dentoalveolar
anchorage presented an average incisor proclination of 4°, while the pendulum with skeletal anchorage showed no variation. Concerning
the effect produced in molars, a greater amount of distalization as a result of inclination was observed in the pendulum with dentoalveolar anchorage (14.1°) in comparison to the one with skeletal anchorage (7.34°).
CONCLUSIONS: with both modalities, the pendulum proved
to be effective for molar distalization; nevertheless, it is important to bear in mind the desired effect on the incisors, as each technique
produces different results.
Key words: pendulum appliance, orthodontic anchorage procedures, dental implants.
INTRODUCTION
Occlusal relationships Class II are characterized by a forward position of the molars and other upper teeth in relation to the lower teeth, and it is usually coupled with increased horizontal overbite. Several genetic and functional factors are related to its etiology, determining skeletal, dentoalveolar and functional alterations in different degrees. Its incidence rate is connected to racial factors. The white race is the most affected1 (22.5%) while the black one is the least affected2 (16.0%); among Latin people it has an incidence of 21.5%3 thus being one of the main reasons for orthodontic consultation.4, 5 In Colombia, it has a prevalence of 20.08%.6
Treatment of this type of occlusal relationships, by complying with the general orthodontic principle of achieving the best possible occlusal relationship with stability and within an esthetically acceptable facial structure, in some cases may require dental extractions,5 but in many other cases it involves moving the first upper molars towards distal and using the extra mesial space to fix dental relationships.
A variety of both intra- and extra-oral mechanoterapies have been suggested for this purpose: extra-oral tractions,7, 8 Wilson's biometric arches,9 repelling magnets,10-12 Herbst,13 Distal Jet,14, 15 Jones Jing,16 Jasper Jumper17, First Class,18 and the like; nevertheless, no single device satisfying all the therapeutic requirements has been found, as several problems persist regarding anchorage loss, movement achievement and patient cooperation.
In 1992, Hilgers introduced the pendulum19 as a therapeutic option for distalizing molars and improving Class II occlusal relationships without performing any extraction, thus obtaining esthetic and functional results with minimum patient participation.
This appliance consists of a Nance button in which two 0,032'' titanium-molybdenum alloy (TMA) springs are inserted in the posterior/lateral portion of the median palatine suture, attached in welded sheaths to the bands of the molars' palatal side. When activated, the springs apply a distalization force on the molars with a pendulum movement, in a wide arch that extends from the center of the palate up to the molars. This pendular movement produces a tendency to cross the bite, and such tendency is controlled by means of a horizontal adjustment handle that neutralizes the movement towards lingual during the molar's distal transposition.
In its original design, reaction forces are transmitted and spread towards the anterior dentoalveolar segment of the anchorage due to the connection of the button to the premolars by means of wire arms either welded to the bands or attached with resin, eventually producing, among other results, an unfavorable effect of mesialization of the premolars, and labialization of the incisors.19-24
An alternative to control the unwanted effects on the teeth consists on skeletal anchorage of the pendulum by directly attaching it to the palate with orthodontic implants, thus obtaining better results.25-33
The objective of this study was to clinically and radiographically establish/compare the effects produced by the pendulum with dentoalveolar anchorage versus skeletal anchorage in relation to the amount and characteristics (rotation, inclination, extrusion) of molar movement and its effect on the anchorage, in patients treated at the Universidad de Antioquia's School of Dentistry, whose treatment plan included distalization of first upper molars.
An additional objective was to provide evidence that supports the use of pendulum in combination with orthodontic implants in order to improve the anchorage and to control negative effects of the appliance.
METHODS
This was a pre-experimental comparative study on a convenience sample composed of 19 subjects aged 13 to 25, ten of whom were being treated with dentoalveolar anchorage pendulum, taken from a sample of a previous study by Betancur et al34, while nine were being treated with skeletal anchorage pendulum. All of the patients met these inclusion criteria: Class II malocclusion without previous orthodontic or orthopedic treatment, periodontically healthy, with adequate oral hygiene habits, and no clockwise mandibular rotation. They should have been prescribed first molars distalization.
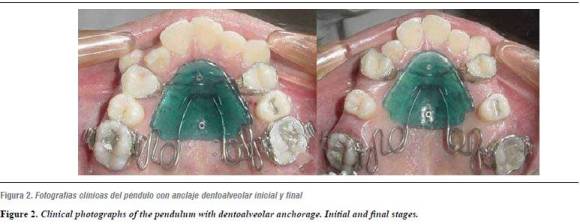
All of the pendulums were made by the same lab technician using the design suggested by Hilgers,19 and it was verified by the lead researcher (figures 1 and 2) . Once the informed consent was signed by the patients and their guardians, installation and activation was initiated.

To perform the skeletal anchorage, Mondeal® titanium screws were used, measuring 11 mm in length and 2 mm in diameter; they were inserted following the protocol established by Tsoun,20 and modified by the surgeon according to each patient's needs. Once anesthesia was adequately applied, the pendulum was placed against the palate, and the screws' localization spots were marked on the acrylic button; extra-orally, perforations were performed on the acrylic with a surgical drill of 1.8 mm in diameter, which provides the perforation with a conical internal shape and the wider base away from tissue. Once the perforated pendulum had been placed against the palate, the surgical drill was used to perform perforations on both soft tissue and cortical bone, with abundant external irrigation of sterile saline solution. Afterwards, the screws were inserted by using a surgical screwdriver. Recommendations and patients' follow-up were performed as suggested by Escobar et al.27
The pendulum was fixed with two screws inserted in the paramedial region, perpendicular to the palate curvature according to each patient's mouth aperture and as posterior as possible, with and oblique arrangement among both. Once the appliance was fixed in its position, the TMA springs were placed in the molars' lingual sheaths by means of a utility clip, and the pendulum was immediately subjected to an orthodontic force of 250 g, which was confirmed by means of a Dontrix (average of the forces used in the clinical studies by Hilgers19 and Ortiz and Gómez).35
None of the patients presented complications before, during or after the procedure of orthodontic implant insertion. During the six-month evaluation period the accessories remained stable in all the patients; just one of them suffered accidental detachment of an implant once the six-month evaluation period had been finished, so that incident was not included in this study as it did not affect the measurements in terms of the clinical or the statistical results.
Removal of distalization appliances was performed by the same operator who installed them; however, the time of detachment was not standard for all the patients (six months) and it varied depending on each case's therapeutic objectives and needs.
Once the appliance was removed, an impression was taken in order to make a Nance holding arch to ensure stability.
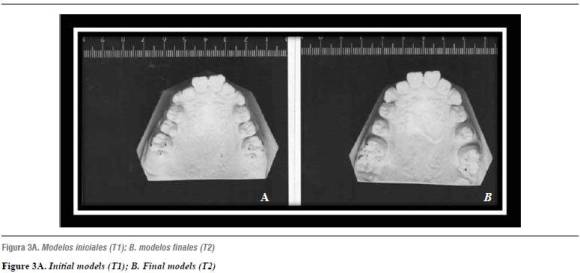
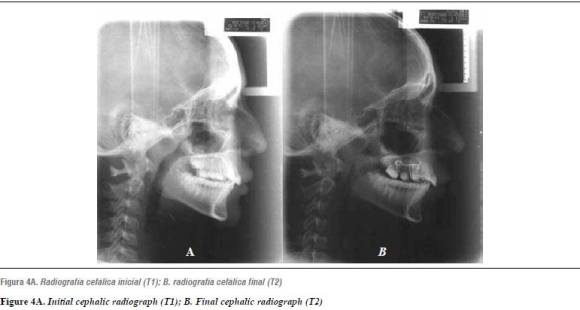
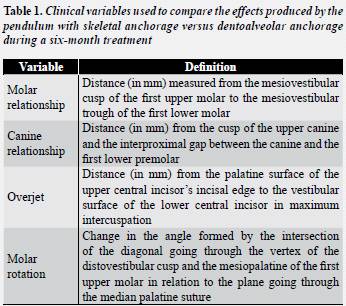
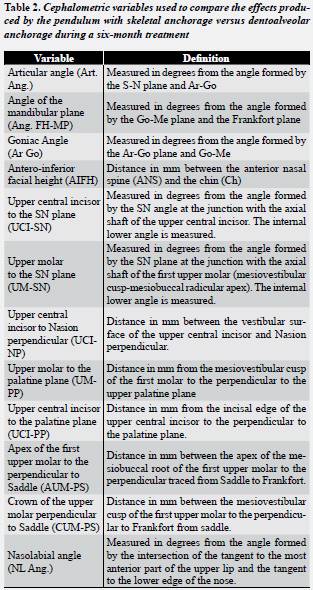
Plaster models were obtained from each patient before inserting the appliances (T1) and six months after treatment (T2) in order to determine changes in the transverse plane (figures 3A and 3B) ; photographs and lateral cephalic radiographs were taken in order to verify changes in the sagittal plane (figures 4A and 4B) Tables 1 and 2 summarize the variables used.
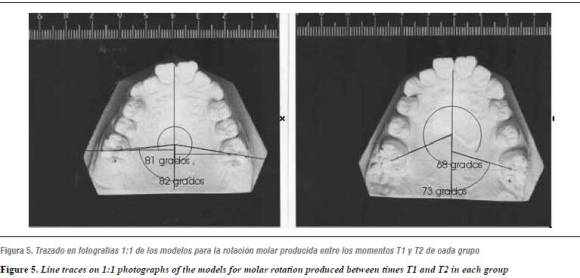
The models were cut at a height of 35 mm, measured from the base to an imaginary plane parallel to the highest occlusal spot in order to obtain standardized occlusal 1:1 photographs. By using a technical pen of 0.05'' in caliber, points were marked in the central cavity as well as in the vertex of the four cusps of the first upper permanent molars. A 200 mm lens and 22 mm diaphragm Nikon camera was used, as well as an Ultra 1800 lamp, Photoshop Adobe 7.0 software, Nikon Capture Control to distance focus-model of 50 cm.
Changes in molar rotation were measured on the models' digitalized photographs by means of the Corel Draw 11 software using the tool that allows measuring angles and following the method used by Betancur et al,23 which indicates that changes from T1 to T2 are measured based on the change at the angle formed by the diagonal that links the apices of the mesiopalatine (MP) or distovestibular (DV) cusps with projection of the sagittal median plane drawn by following the palatine median raphe (figure 5).
A clinical follow up was performed every four weeks in order to weigh up the arms' activation force and to register molar relationship changes, canine relationship and horizontal overbite (measured between the right lower and upper incisors and at the mesiodistal half of the incisal edge at the level of 11/41 and 21/31).
This measurement was performed with a digital Discover® calibrator; in the same session, activation of the spring was checked and it was reactivated to 250 g in order to maintain force level. The findings were recorded on forms previously designed for this purpose and they were consolidated in tables.
Moreover, a standard digital photograph series was taken at the beginning and the end of the study in order to provide evidence of the follow up in each case. Three extra-oral photographs were included: front view, right profile, and smile, as well as five intraoral photographs: superior and inferior arches, right and left lateral views, and frontal occlusion. The standardization parameters for the photographs were as follows:
A 35 mm Nikon camera placed on a stand for reproductions.
Lighting: direct main light, flash ultra 1800 white lightning.
Zoom of 75-150, with a focus length of 135 mm.
Exposure time: 1/605.
F-22 diaphragm for ISO 100.
Once the observation period was completed, patients continued their treatment at the clinics of Universidad de Antioquia's School of Dentistry according to the indications for each case.
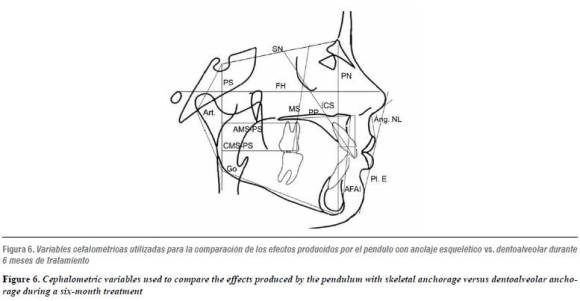
The lateral cephalic radiographs were digitalized by means of a transparency flatbed Epson V 700 photo scanner, which enables 1:1 scanning of the radiographs. The Radiocef 2 cephalometry software was also used (figure 6). All the dots were made by the same operator, who was subjected to the Pearson's correlation test in order to determine error level, finding out that calibration was statistically significant (coefficient r = 0.996, p < 0.05).
The data obtained during the clinical and radiographic evaluations were transferred to an Excel® sheet and analyzed by means of the SPSS 17.0® statistics software.
STATISTICAL ANALYSIS
In the first place, a descriptive analysis of the clinical and radiographic variables was performed by means of central and dispersion tendency measures: average and standard deviation for each group.
Then, the Shapiro-Wilk test was applied in order to validate the variables' assumption of normality. Due to the sample size, some of the variables did not conform to this assumption (Rot. Mol. Left T2, UCI-NP T2, AUM-PS T1); therefore, non-parametric tests were used for the statistical analysis. The Wilcoxon test for paired samples was used in order to establish the changes occurred in both clinical and radiographic variable means between the times (T1) and (T2) in each group; and the Mann-Whitney U test for independent samples was used in order to determine differences between both clinical and radiographic variable means in both groups (dentoalveolar and skeletal anchorage). For all the statistical tests, a significance level of 5% was considered (P < 0.05).
RESULTS
The molar relationship changes that occurred 6 months after treatment with either dentoalveolar anchorage pendulum or skeletal anchorage pendulum are shown in table 3.
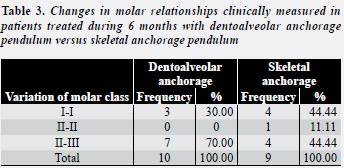
In all the cases, molar distalization may be observed, advancing from a molar relationship Class II to Class I, or overcorrecting to Class III, except for one case of the group of pendulum with skeletal anchorage that remained in Class II, with a change from Class II at 6 mm to Class II at 1.7 mm.
tables 4 and 5) summarize the changes of the clinical variables evaluated: overjet and molar rotation of the pendulums with dentoalveolar and skeletal anchorage.
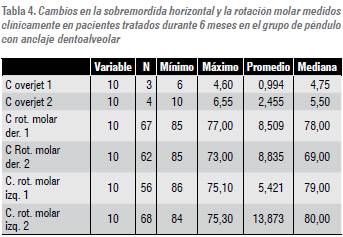
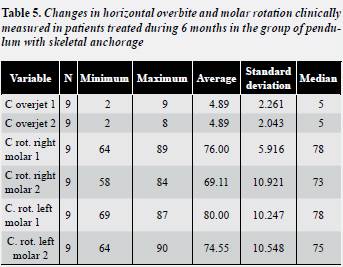
The overjet found in the clinical evaluation of the pendulum with dentoalveolar anchorage increased and average of 2 mm between T1 and T2, while the pendulum with skeletal anchorage remained unchanged.
Concerning molar rotation, the two treatment groups presented both mesiovestibular rotation (+) and mesiopalatine rotation (—); nevertheless, the final average in both cases indicates positive rotations.
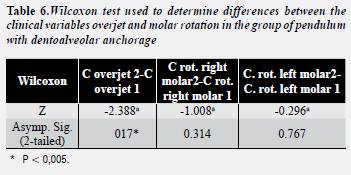
The Wilcoxon test applied to the clinical variables was intended to find significant differences between T1 and T2 in each group, and it showed statistically significant changes (P < 0.05) only in the overjet measurement of the subjects treated with dentoalveolar anchorage pendulum (table 6) .
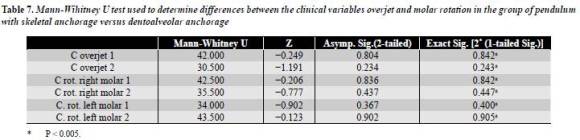
The Mann-Whitney U test was used to compare the medians of the clinical variables of both groups, and it proved that there were no statistical evidence that confirmed a greater effect on the incisors and molars of one pendulum or the other (table 7).
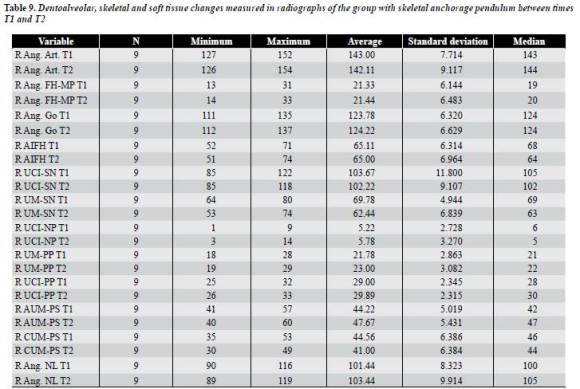
Dentoalveolar, skeletal and soft tissue changes cephalometrically found in T1 and T2 in both groups are observed in tables 8 and 9).
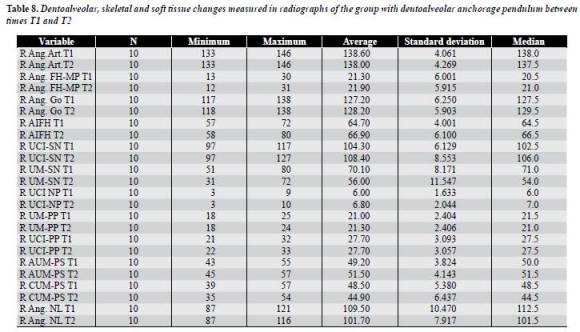
Although no statistical significant difference was found between T1 and T2 in these variables: articular angle, mandibular plane angle, and goniac angle, a slight decrease is observed in the first angle and a slight increase in the other two.
The position of the upper incisor, represented by the angle UCI-SN, notably varied in the group treated with dentoalveolar anchorage pendulum, showing an average vestibular inclination increase of 4° between T1 and T2, while in the group treated with skeletal anchorage it showed an average decrease of 1.4°.
Vertically, upper incisor position change was evaluated by means of the difference between T1-T2 of the variable UCI-PP, which did not show significant variation in any group.
Concerning the upper molars sagittal position change, it could be observed that distal displacement of the crown, measured by means of the CUM-PS distance between T1 and T2 for the group with dentoalveolar anchorage, was 3,6 mm ± 1.05 in average, with a median of distal inclination of 14.1°, measured by means of the UM-SN angle. While in the group with skeletal anchorage a distalization average of 3.56 ± 0.915 was observed, with inclination median of 7.34°.
In the vertical dimension, measurement of molar position change was obtained by comparing T1 and T2 in terms of UM-PP distance in each group.
The group of pendulum with dentoalveolar anchorage did not show vertical position variation, while the one of pendulum with skeletal anchorage presented a slight tendency to extrusion with an average of 1.2 mm.
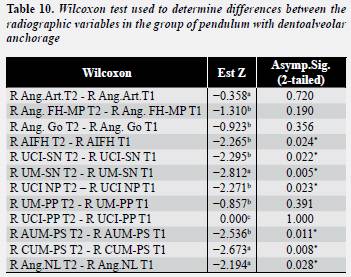
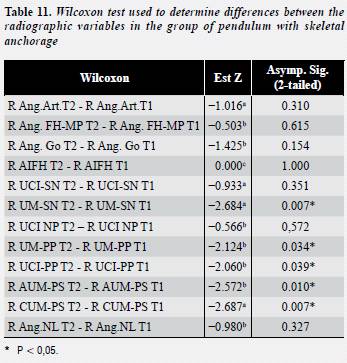
The Wilcoxon test applied at the radiographic variables established significant statistical differences between times T1 and T2 for each treatment group. In both groups, statistical evidence of differences between T1 and T2 was found in these variables: UM-SN, AUM-PS, CUM-PS. Besides, in the group with dentoalveolar anchorage, in these variables: AIFH, UCI-SN, UCI-NP and NL Ang. (table 10) and in the group with skeletal anchorage in the variables UM-PP and UCI-PP (table 11).
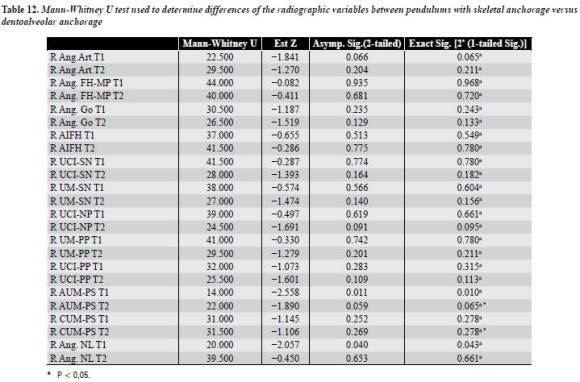
The Mann-Whitney U test, applied on the radiographic variables with a significance level of 5%, showed significant statistical differences in these variables: AUM-PS in T1 and NL Ang. in T1 (table 12).
DISCUSSION
This study makes a clinical and radiographic comparison of the dentoalveolar effects produced by the pendulum with dentoalveolar anchorage versus skeletal anchorage.
Comparison of the effects produced by these two appliances is the object of study of several research projects,34-38 some of which are listed in table 13.
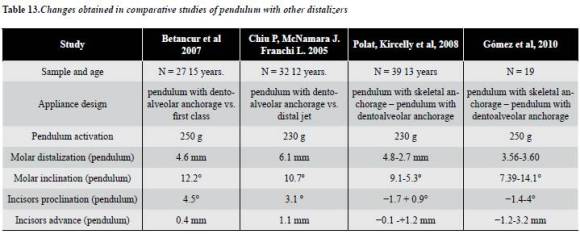
When comparing the pendulum in the two anchorage techniques, one may conclude that both pendulums produce a great amount of distal crown inclination of the molars without significant statistical differences; however, the difference is that while the pendulum with a dentoalveolar support presents effects of proclination on the anchorage area, the pendulum with skeletal anchorage presents a tendency to retroincline upper incisors in relation to the base of the skull, without changes in the palatine plane (figure 6).
The average distalization amount produced by the pendulum with dentoalveolar anchorage was 3.6 mm (as measured in this study) while the average distalization produced by the pendulum with skeletal anchorage was 3.56 mm.
The distalization results of this study agree with the ones of the study by Betancur et al, who found out distalization of 4.68 mm.34 As it is the same sample, the difference may be due to lack of calibration of the operators who measured both studies. Conversely, Chiu, McNamara and Franchi found 6.1. mm of distalization,36 while Donald et al found out a distal movement of 0.8 mm in a treatment period of 28 months.38 These differences with our study may be due to variations in the characteristics of the samples used, the amount of force applied at the beginning of the study, and different methods of measurement.
In 2006, Hancioglu et al conducted a study on 39 patients, comparing the effects produced by the pendulum anchored in implants and with dentoalveolar anchorage. Among their observations, they found out a greater amount of distalization in the pendulum with skeletal anchorage (4.8 mm) than that with dentoalveolar anchorage (2.7 mm), besides 0.9° of incisors proclination in the pendulum with dentoalveolar anchorage and 1.7° incisors retoinclination in the pendulum with skeletal anchorage.28 Similarly, the present study also found incisors inclination of 1.4° in the group with skeletal anchorage, thus agreeing with the results of the study by Escobar et al, who found out a palatine inclination of 2.5 ± 2.98°,27 as well as with the findings by Oberti et al,39 whose lingual incisors inclination was of 0.84 ± 1.41°; nevertheless in the group of pendulum with dentoalveolar anchorage a proclination of 4° was observed, being bigger than the one reported by Hancioglu et al. The differences among these studies may be due to dissimilar reference frames used. Besides, the present study found out less distalization in the group with skeletal anchorage compared to the study by Hancioglu; this result may be related to the predominance of counter-clockwise mandibular rotation in the groups of this study, which could have been coupled with hypertonicity of masticatory and perioral muscles, as observed in the clinical assessment of the subjects, which in turn could have resulted in limitation of the molars' posterior movement.
Concerning the amount of upper incisors retroinclination found out in the group with skeletal anchorage, it agrees with the results of other studies,27-31 which do not present incisors proclination, thus proving the efficiency of anchorage systems supported on implants.
The clinical evaluation considered changes in terms of overjet, molars rotation, and variations of molar and canine relationships.
Although no significant statistical differences were observed in molar rotation, clinical predominance was found in terms of mesiovestibular rotation in both types of anchorage, thus agreeing with the studies by Betancur et al and Byloff and Darendeliler.24, 34
As a result of the treatment with pendulum of dentoalveolar anchorage, increase of AIFH was found in the present study, consistent with the studies by Hilgers, Byloff, and Betancur.19, 25, 34 Nevertheless, this increase would have been expected to be the result of extrusion of the upper molars but, on the contrary, a slight intrusive movement occurred caused by greater molar inclination; also, the articular angle decrease that was observed suggests that these AIFH changes occur because of growth. Another factor to consider in relation to AIFH increase in the group treated with pendulum of dentoalveolar anchorage versus skeletal anchorage is that the age range in the first group is 12 to 16 years, with an average of 13 years, while in the second one the age range is 13 to 25 years, with an average of 17.5 years, which suggests that AIFH increase in these subjects was not the result of dentoalveolar compensation but expression of their growth patterns.
With regard to upper molar movement as a result of the pendulum with dentoalveolar anchorage, greater distal inclination of the crown (14.1°) was found in comparison to the pendulum with skeletal anchorage (7.34°), thus concurring with the studies by Chiu, Betancur, Polat-Ozsoyand other studies.34, 36-38 Also, greater molar extrusion occurred with the latter, maybe as a consequence of molar projection towards gingival and due to the molar's greater coronal inclination towards distal in the case of the pendulum with dentoalveolar anchorage.
It is important to note the mesialization of the upper molar mesiovestibular root apex observed in the two groups of our study, being greater in the group of skeletal anchorage (3.54 mm) compared with the group of dentoalveolar anchorage (2.3 mm).This was probably an effect of the monthly reactivation of the appliance force, which could have enabled the expression of the moment-force relation needed.
Just like the studies by Hilgers, Butchart, Wong, Angelieri, Byloff, and others, we found out greater upper incisor proclination in relation to the base of the skull, with an increase of 4°, in the group of dentoalveolar anchorage.19, 21-24 This might be the result of diverse control at the site of anchorage between the two pendulum systems studied. Although no significant statistical differences were found in terms of overjet when comparing the two pendulums, a substantial clinical difference may be observed in the effect produced by the pendulum with dentoalveolar anchorage (an increase of 2 mm) compared to the pendulum with skeletal anchorage (an increase of 0 mm).This confirms the findings of other studies such as the ones by Buchart,21 Angelieri,23 and others.22, 24, 25
As a result of greater upper incisor proclination in this group, an increase of 7.8° in the nasolabial angle was observed, agreeing with the study by Betancur et al.34
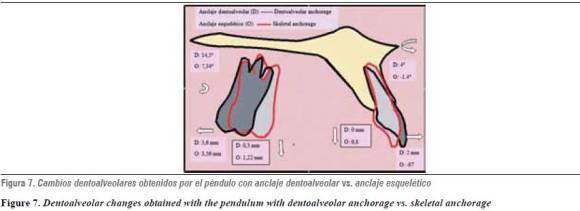
The predominant molar rotation in both systems was the mesiovestibular. The amount of distalization was similar in both pendulums; however, greater upper molar distal inclination may be observed in the pendulum with dentoalveolar anchorage (figure 7).
CONCLUSIONS
Based on the studied sample and with the conditions of appliance use of this study, it may be concluded that:
In any of the two anchorage systems, the pendulum is an effective treatment for molar distalization, especially in terms of distal coronal inclination movement.
The pendulum with dentoalveolar anchorage produces vestibularization of upper incisors; although it is not statistically significant, from a clinical point of view some significant differences were observed (4° and 2 mm).
The pendulum with skeletal anchorage does not produce overjet clinical changes.The radiographic analysis showed upper incisors retroinclination movement of 1.4°.
The pendulum with dentoalveolar anchorage produces more molar distal inclination (14.5°) but less mesial displacement of the molar radicular apex in comparison to the pendulum with skeletal anchorage (7.34°).
There are no significant statistical differences in terms of molar rotational behavior in both types of anchorage.
Although no significant statistical differences were found between the distalization devices studied, it maybe suggested that the pendulum with skeletal anchorage is more efficient for ''en masse'' molar distalization movement and it has a smaller proinclination effect on the upper molars, under the conditions of the sample of this study.
CORRESPONDING AUTHOR
Sandra Liliana Gómez
Facultad de Odontología
Universidad de Antioquia
Correo electrónico: sandraligomez@une.net.co
REFERENCES
1. Horowitz HS, Doyle BS. Occlusal relation in children born and reared in an optimally flouridated community. Angle Orthod 1970; 40(2): 104-111. [ Links ]
2. Garner LD, Butt MH. Malocclusion in black Americans and Nyeri Kenians. Angle Orthod 1985; 55(2): 139-146. [ Links ]
3. Silva RG, Kang DS. Prevalence of malocclusion among Latino adolescents. Am J Orthod Dentofacial Orthop2001; 119(3): 313-315. [ Links ]
4. Moyers RE. Clasificación y terminología de la maloclusión. Diagnóstico. Manual de ortodoncia. 4.ª ed. Buenos Aires: Panamericana; 1992. [ Links ]
5. Mattijs JP, Stalpers A, Johan W, Booij B, Ewald M, Bronkhorst C et al. Extraction of maxillary first permanent molars in patients with Class II division 1 malocclusion. Am J Orthod Dentofacial Orthop 2007; 132: 316-323. [ Links ]
6. Thilander B, Pena L, Infante C, Parada S, de Mayorga C. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogotá, Colombia. An epidemiological study related to different stages of dentoalveolar development. Eur Orthod J 2001; 23(2): 153-167. [ Links ]
7. Graber TM. Extraoral force-facts and fallacies. Am J Orthod 1955; 41: 490-505. [ Links ]
8. Kirjavainen M, Kirjavainen T, Haavilkko K. Changes in dentoalveolar arch dimensions by use of an orthopedic cervical headgear in class II correction. Am J Orthod Dentofacial Orthop 1997; 111: 59-66. [ Links ]
9. WilsonWL. Modular Orthodontic system part I. J Clin Orthod1978; 12(4): 259-78. [ Links ]
10. Gianelly AA, Vitas AS, Thomas WM, Berger OG. Distalization of molars with repelling magnets. J Clin Orthod 1988; 22: 40-44. [ Links ]
11. Blechman AM. Magnetic force system in orthodontics. Clinical results of a pilot study. Am J Orthod Dentofacial Orthop 1985;87: 201-210. [ Links ]
12. Gianelly AA, Viatas AS, Thomas WM. The use of magnets to move molars distally. Am J Orthod Dentofacial Orthop 1989; 96: 161-167. [ Links ]
13. Pancherz H. History, background, and development of the Herbst appliance. Semin Orthod 2003; 9: 3-11. [ Links ]
14. Carano A, Testa M, Siciliani G. The Distal Jet for uprighting lower molars, J Clin Orthod 1996; 30: 707-710. [ Links ]
15. Carano A, Testa M. The Distal Jet appliance for upper molar distalization. J Clin Orthod 1996; 30: 374-380. [ Links ]
16. Runge ME, Martin JT, Bukai F. Analysis of rapid maxillary molar distal movement without patient cooperation. Am J Orthod Dentofacial Orthop 1999; 115: 153-157. [ Links ]
17. David A, Covell JR, Dennis W, Trammell, Roger P, Richard W. A cephalometric study of Class II division 1 malocclusions treated with the Jasper Jumper Appliance. Angle Orthod 1999; 69(4): 311-320. [ Links ]
18. Fortini A, Lupoli M, Parri M. The first class appliance for rapid molar distalization. J Clin Orthod 1999; 33: 322-328. [ Links ]
19. Hilgers JJ. The pendulum appliance for Class II noncompliance therapy. J Clin Orthod 1992; 26: 700-713. [ Links ]
20. Tsoun T, Keles A, Everdi N. Method for the placement of palatal implants. Int J Oral Maxillofac Implants 2002; 17(1): 95-100. [ Links ]
21. Butchart J. An evaluation of the pendulum distalizing appliance. Sem Orthod 2000; 6: 129-135. [ Links ]
22. Wong A, Rabie A. The use of pendulum appliance in the treatment of Class II malocclusion. Br J Orthod 1999; 187(7): 367-370. [ Links ]
23. Angelieri F, Rodrigues R, Rodrigues M, Fuziyd A. Dentoalveolar and skeletal changes associated with the pendulum appliance followed by fixed orthodontic treatment. Am J Orthod Dentofacial Orthop 2006; 129: 520-527. [ Links ]
24. Byloff FK, Darendeliler MA. Distal movement molar using the pendulum appliance. Part 1: clinical and radiological evaluation. Angle Orthod 1997; 67(4): 249-260. [ Links ]
25. Byloff FK, Darendeliler MA. Distal movement molar using the pendulum appliance. Part 2: The effects of maxillary molar root uprighting bends. Angle Orthod 1997; 67(4): 261-270. [ Links ]
26. Ahmet K, Nejat E, Serdar S. Bodily distalization of molars with absolute anchorage. Angle Orthod 2003; 73(4): 471-482. [ Links ]
27. Escobar SA, Tellez PA, Moncada CA, Villegas CA, Latorre CM, Oberti G. Distalization of maxillary molars with the bone supported pendulum: a clinical study. Am J Orthod Dentofacial Orthop 2007; 131: 545-549. [ Links ]
28. Hancioglu B, Ozgur P, Kircelly C. Maxillary molar distalization with a bone anchored pendulum appliance. Angle Orthod 2006; 76(4): 650-659. [ Links ]
29. Oncag G, Akyalcin S, Arikan F. The effectiveness of a single osteointegrated implant combined with pendulum springs for molar distalization. Am J Orthod Dentofacial Orthop 2007; 131(2): 277-284. [ Links ]
30. Choi B, Zhu S, Kim Y. A clinical evaluation of titanium miniplates as anchor for orthodontic treatment. Am J Orthod Dentofacial Orthop 2005; 128(3): 382-384. [ Links ]
31. Seung-Min Lim; Ryoon-Ki Hong. Distal movement of maxillary molars using a lever-arm and mini-implant system. Angle Orthod 2008; 78(1): 167-175. [ Links ]
32. Roberts WE, Smith RK, Silberman Y, Mozsary PG, Smith RS. Osseous adaptation to continuous loading of rigid endosseous implants. Am J Orthod Dentofacial Orthop 1984; 86: 95-111. [ Links ]
33. Roberts WE, Marshall KJ, Mozsary P. Rigid endosseous implant utilized as anchorage to protract molars and close atrophic extraction site. Angle Orthod 1990; 60: 135-152. [ Links ]
34. Betancur JJ, Carvajal A, Jaramillo PM, García J, Madrigal N, Lopera M. Estudio comparativo del efecto clínico producido por el FirstClass® y el péndulo en pacientes atendidos en la Facultad de Odontología de la Universidad de Antioquia: análisis radiográfico y de modelos. Rev Fac Odontol Univ Antioq 2007; 18(2): 29-42. [ Links ]
35. Ortiz L, Gómez L. Efecto de tres diseños de péndulo sobre la generación de fuerza producida a diferentes grados de activación y desactivación. Un estudio in vitro. Revista CES Odontol 2001; 14(2): 35. [ Links ]
36. Chiu PP, McNamara JA, Franchi L. A comparison of two intraoral molar distalization appliances: Distal jet versus pendulum. Am J Orthod Dentofacial Orthop 2005; 128(3): 353-365. [ Links ]
37. Polat-Ozsoy, Kircelli H, Özçirpici Z, Özgür P, Uçkand S. Pendulum appliances with 2 anchorage designs: Conventional anchorage vs. bone anchorage. Am J Orthod Dentofacial Orthop 2008; 133: 339.e9-339.e17. [ Links ]
38. Donald R, Burkhar DT, McNamara J, Baccetti T. Maxillary molar distalization or mandibular enhancement: a cephalometric comparison of comprehensive orthodontic treatment including the pendulum and the Herbst appliances. Am J Orthod Dentofacial Orthop 2003; 123: 108-116. [ Links ]
39. Oberti G, Villegas C, Ealo M, Palacio J, Baccetti T. Maxillary molar distalization with the dual-force distalizer supported by mini-implants: a clinical study. Am J Orthod Dentofacial Orthop 2009; 135: 282.e1-282.e5. [ Links ]
