










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkUniversitas Psychologica
Print version ISSN 1657-9267
Univ. Psychol. vol.13 no.4 Bogotá Oct./Dec. 2014
https://doi.org/10.11144/Javeriana.UPSY13-4.efds
Executive Function Deficits and Symptoms of Disruptive Behaviour Disorders in Preschool Children*
Déficits en la función ejecutiva y síntomas de trastornos disruptivos de la conducta en niños preescolares
Eva Angelina Araujo Jiménez**
Universidad Autónoma de Sinaloa, Culiacán, México
Ma. Claustre Jané-Ballabriga***
Albert Bonillo Martin
Connie Capdevilla i Brophy
Universitat Autònoma de Barcelona, España
*Agradecimientos: El trabajo tuvo la colaboración del Equip d'Assessorament i orientació Psico-pedagògica d'Osona, EAP, y fue financiado por los Fondos de Investigación Sanitario FIS número 070027.
**E-mail: eva.araujo.j@gmail.com
***E-mail: mariaclaustre.jane@uab.cat, albert.bonillo@uab.cat, ConnieCapdevila@copc.cat
Recibido: diciembre 13 de 2013 | Revisado: diciembre 13 de 2013 | Aceptado: abril 9 de 2014
Para citar este artículo
Araujo, E. A., Jané-Ballabriga, M., Bonillo, A., & Capdevilla, C. (2014). Executive function deficits and symptoms of disruptive behaviour disorders in preschool children. Universitas Psychologica, 13(4), 1267-1277. http://dx.doi.org/10.11144/Javeriana.UPSY13-4.efds
Abstract
The Executive Function is a set of cognitive processes that are developed from the earliest ages. Recent studies in children with disruptive behaviour disorders suggest the presence of effects on the executive functioning. The aim of this study is to know the association among symptoms of Attention Deficit with Hyperactivity Disorder, Oppositional Defiant Disorder, and Conduct Disorder, and Executive Function in children from 3 to 6 years old. Method: A descriptive cross-sectional study was conducted. An assessment was performed on a sample of 444 subjects from Spain; it was made through an inventory for parents and teachers to estimate the capacity of Executive Function. Results: a relation between the symptoms of Attention Deficit with Hyperactivity Disorder, Oppositional Defiant Disorder, Conduct Disorder, and the Executive Function deficit was found. The presence of symptoms of Attention Deficit with Hyperactivity Disorder inattentive type is associated with deficiencies in all areas of Executive Function, which does not occur with other symptoms. Conclusion: It is important to know the specific characteristics of each symptomatology by taking into account their executive functioning, in order to achieve accurate diagnoses in the clinical setting, as well as appropriate therapy according to the deficiencies presented by children.
Keywords :Executive function; ADHD; Disruptive Behaviour Disorders; preschool children
Resumen
Las funciones ejecutivas son un conjunto de procesos cognitivos que se desarrollan desde los estadios iniciales. Recientes estudios en niños con trastorno de comportamiento adaptativo sugieren la presencia de efectos sobre el funcionamiento ejecutivo. El objetivo del presente trabajo es conocer la asociación entre síntomas del síndrome por déficit de atención con hiperactividad, síndrome opositivo desafiante y trastorno de conducta y función ejecutiva en niños de 3 a 6 años. La investigación de tipo descriptivo transversal se llevó a cabo sobre una muestra de 444 niños españoles. Para estimar la capacidad de funciones ejecutivas, se estructuró un inventario para padres y educadores. Se encontró una relación entre los síntomas del síndrome de défict de atención con hiperactividad, síndrome opositivo desafiante y trastorno de conducta, y déficit en funciones ejecutivas. La presencia de los síntomas del síndrome de défict de atención con hiperactividad de tipo inatento se asoció con deficiencias en todas las áreas de funciones ejecutivas, lo que no ocurre con otros síntomas. Por lo tanto, es importante conocer las características específicas de cada sintomatología, tomando en cuenta su funcionamiento ejecutivo, con el ánimo de lograr diagnósticos adecuados en el ámbito clínico y la terapia apropiada acorde a las deficiencias presentadas en niños.
Palabras clave :Funciones ejecutivas; síntomas del síndrome de défict de atención con hiperactividad; trastorno de conducta adaptativa; preescolar; niños
Executive Function (EF) is a set of higher-order cognitive processes and emotional and motivational skills, mediated by the prefrontal cortex of the brain (Trujillo & Pineda, 2008; Welsh, Pennington, & Groisser, 1991), which aims to help a person to lead and guide the behaviour to reach a goal (Wâhlstedt, Thorell, & Bohlin, 2008), as well as to regulate it against possible changes in his/her immediate context (Goldberg, 2002). This function also regulates the cognitive, emotional, and social behaviour of individuals (Anderson, 2002; Barkley, 2000; Goldberg, 2002; Senn, Espy, & Kaufmann, 2004). EF includes functions such as directing attention, pattern recognition of priority, goal formulation, activity planning, plan implementation, self-regulation, inhibitory control, flexibility, and self-evaluation of the results from the performed action (Senn et al., 2004). The importance of EF in daily life is expressed in educational achievement and behavioural adjustment of children in the context where they develop (Biederman et al., 2004; Clark, Pritchard, & Woodward, 2010; Mattison & Mayes, 2012).
From early age, children develop executive activities (Isquith, Crawford, Espy, & Gioia, 2005), and manage to achieve different progressive goals as they pass through developmental stages (Goldberg, 2002). Thus, when children are between 3 to 6 years old (preschool age), they acquire the ability to follow rules, which would lead to executive activities such as inhibitory control, self-regulation, emotional control, and problem solving (Espy, Sheffield, Wiebe, Clark, & Moehr, 2011). Before 5 years old, children make too many mistakes during problem-solving, since they are not able to change the rules according to different tasks. Trujillo and Pineda (2008) state that problem solving is the cornerstone to developing EF, since it leads to the implementation of complex strategies. However, after school age (6 years) the child carries out more complex executive activities. These skills reach full development years later (Goswami, 2002).
Isquit et al. (2005) argue that preschool children are not yet able to completely control their emotional executive functions, as well as their behavioural ones. When studying the EF in this age group, it is necessary to note that results may vary depending on the level of cognitive development of children. Espy et al. (2011) report that in order to assess EF in preschoolers, age-appropriate behaviours should be differentiated from impaired behaviours. For instance, the lack of attention in preschoolers may be a characteristic of the child, as well as a deficiency in his/her EF. Despite this difficulty in distinguishing between the variations of the stages of development and a deficit, many researchers focus on the study of cognitive abilities in infants, since these are the roots of the various disorders that manifest in childhood and adolescence, v.g. Attention Deficit Hyperactivity Disorder (ADHD), autism, Oppo-sitional Defiant Disorder (ODD), among others (Isquith et al., 2005).
From the EF study in preschoolers, researches are conducted to observe the impairments of EF in the disruptive behaviour disorders, such as ADHD, ODD, and Conduct Disorder (CD), since some authors (Mullane, Corkum, Klein, McLaughlin, & Lawrence, 2011; Schoemaker et al., 2012) have found that ADHD, ODD, and CD are associated with a poor adaptive behaviour. An accurate study of these disorders in preschool children is of great interest because their symptoms can be detected at an early age and because they can also be comorbid (Sonuga-Barke, Dalen, Daley, & Remington, 2002; Thorell & Wâhlstedt, 2006). It has been demonstrated that children who show symptoms of psychiatric disorders at an early age, but who do not meet the diagnosis of a particular disorder, are also impaired in their psychosocial functioning, such as the diagnosed children (Wâhlstedt et al., 2008).
ADHD is one of the most common disorders in children. It is characterized by a persistent and extreme pattern, including inattention, hyperactivity, and impulsivity, which cause significant impact on school, work, family, and social contexts of the impaired person (American Psychiatric Association [APA], 2000). Some studies have found strong correlation between EF dysfunctions and ADHD symptoms in children (Brocki, Eninger, Thorell, & Bohlin, 2010; Mullane et al., 2011; Sonuga-Barke et al., 2002). Recent studies (Clark, Prior, & Kin-sella, 2002; Fischer, Barkley, Smallish, & Fletcher, 2005; Wâhlstedt et al., 2008) have found that ADHD symptoms along with EF impairments are early predictors of continued disruptive behaviour disorders due to features such as inattention, poor impulse control, and poor planning ability.
Other studies (Barkley, 1998; Brocki et al., 2010; Gambin & Swiçcicka, 2009; Sonuga-Barke et al., 2002; Wâhlstedt et al., 2008) agree that, usually, the ADHD symptoms occur simultaneously with behavioural inhibition. But working memory and flexibility are also affected (Brocki et al., 2010; Re, De Franchis, & Cornoldi, 2010). According to Brocki et al. (2010), children with inattention have more deficits in the EF than children with hyperactivity/impulsivity.
As for ODD, it is characterized by an attitude of hostility and rejection toward figures representing authority, which leads to opposition and disobedience of the accepted guidelines and criteria of home, school, and social relationships (APA, 2000). For its part, CD is characterized by the transgression of the accepted social norms as accorded by a group, which regulate the relations of its members. Children with CD are aggressive, antisocial, and deeply disturbing to others (18). There are few studies that explore the executive function of both disorders, and some have found weaknesses in their executive functions. Van Gooze et al. (2004) state that although there is no strong evidence of these deficiencies in children with these disorders, those who suffer ODD and CD have problems to self-regulate their emotions and motivations. Sergeant, Geurts, and Oosterlaan (2002) and Raaijmakers et al. (2008) found that deficits in EF, like lack of inhibition, are present in both ODD and CD. Other studies (Qian, Shuai, Cao, Chan, & Wang, 2010) mention that people with ODD and CD have no difficulty in their EF. Thorell and Wâhlstedt (2006) argue that deficits in EF in children with ODD are due to an overlap of ODD and ADHD.
Sergeant et al. (2002) state that ADHD, ODD and CD have the same deficits in EF. Thus, Van Gooze et al. (25) propose a more detailed differentiation of executive dysfunction in these disruptive behaviour disorders, since there are few studies that give information about the deficits in EF of each symptomatology. Thus, at present there is no agreement among scholars on the topic of EF differences in disruptive behaviour disorders.
From the above researches, we believe that knowing the association between symptoms of disruptive behaviour disorders and EF deficits is important, especially at an early age, since at this age future aggressive behaviour may be prevented (Wâhlstedt et al., 2008). Some studies indicate that children with disruptive behaviour disorders have more emotional, motivational and social skills problems when they present deficits in their EF (Biederman et al., 2004).
The aims of this study are to evaluate children's EF with ADHD, ODD, and CD symptoms; to know what disorders are most affected by executive dysfunctions; and to differentiate the information of parents from that of teachers. As hypotheses we hope to find significant differences in the EF of the various disorders; to agree with the literature, in that the three disruptive behaviour disorders show global executive dysfunctions, and in that children with symptoms of ADHD-I type have greater involvement in executive processes.
Method
Participants
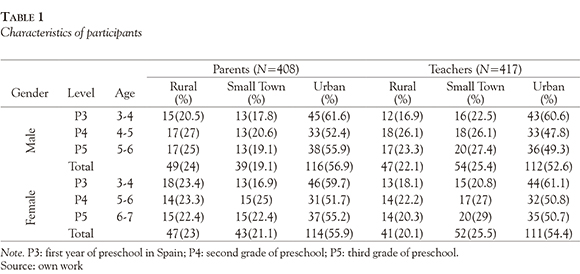
The sample consisted of444 children aged between 3 and 6 years old (See Table 1). From a random cluster sampling, the study included 13 pre-schools of the Osona region, in Spain, that met the requirement of having 1 or 2 lines of early childhood education (participants represented 10% of the Osona's population between 3-6 years of age). Five schools refused to participate, but they were replaced with the same procedure. 408 parents (92%) and 417 teachers (94%) answered the questionnaire with lower values than the critical ones in the validity scales (negativity, 100% of parents and 96.6% of teachers; and inconsistency, 95.5% of parents and 96.8% of teachers). They answered an instrument to assess symptoms present in children and another to assess executive function. For more information please see Bonillo, Araujo, Jané, Capdevila, and Riera (2011).
Measures
Assessment of Executive Function
Behaviour Rating Inventory of Executive Function-Preschool Version (Bonillo et al., 2011; Gioia, Espy, & Isquith, 2003), which comprises a questionnaire for parents and one for teachers. They both were designed to assess EF. Each questionnaire has 63 items divided into 5 clinical scales - and 2 validity scales -, which form 3 broader indexes: inhibitory self-control, flexibility, and emergent metacognition, and a Global Execution combined score. They are coded into a three-points scale: 1 = Never; 2 = Sometimes; and 3 = Often. The 5 clinical scales are: Inhibition, Shift, Emotional Control, Working Memory and Plan/Organize.
The BRIEF-P was standardized and validated to be used with children 2 to 5 years 11 months old. The BRIEF-P has a strong validity, since items were selected from clinical interviews.
Presence of symptoms of disruptive behaviour disorders
Early Childhood Inventory: Parent and Teacher Checklist, ECI-4 (Sprafkin & Gadow, 1996; Viñas et al., 2008). Is an instrument designed to screen for the symptoms of psychiatric disorders in children from 3 to 6 years of age. The items comprising it are based on the diagnostic criteria of the DSM-IV (APA, 2000). Each item (symptom) is valued by parents and teachers in a four-point scale (never = 0, sometimes = 1, often = 2, very often = 3). The ECI-4 categories can be assessed in two different ways: Screening Cutoff and quantification of the severity of symptoms. The latter is the one that we used in our study. The applied version (Viñas et al., 2008) was previously adapted and validated for the Spanish population, with a generally satisfactory internal consistency for parent-teacher version (a of 0.67 to 0.93) but lower for emotional disorders (a of 0.46 to 0.65).
Procedure
At first, the Equip d'Assessorament i Orientació Psi-copedagògica dOsona [Osona's Psychopedagogical Counselling Team] (EAP) granted permission and agreed to participate in the study. The EAP contacted the management team of each school for the acceptance of participation. Parents were asked to sign an informed consent. Teachers gave the questionnaires to parents, and the latter gave them back to the school. Once collected all the questionnaires, each school, by means of its principal, gave them to the EAP member responsible for his area.
Data analysis
For the evaluation of the BRIEF-P it was used the SPSS software for Windows, version 18.0. Using the general statistical model of multiple linear regression, it was analyzed the statistical relationship between each of the scales of the BRIEF-P (dependent variables: Inhibition, Shift, Emotional Control, Working Memory, Plan/Organize), and symptoms of ADHD, ODD, and CD as scored by the ECI-4 (independent variables). Each informant realized the evaluation separately: parents and teachers. The "Backward" was the method of calculation used each model. It successively eliminates insignificant variables until obtaining a final model in which all predictors are statistically significant.
Standardized coefficients (or Beta) were observed on each independent variable to determine the relative importance of each variable of the BRIEF-P on the ECI-4 scores in standard deviation units, direct scores. Since the models are explanatory models, i.e., they are intended to measure the effect of some variables on others; the confusion inherent in non-experimental studies was minimized. The adjustment variables were sex and age, and their effects were controlled by incorporating them into the multiple regression calculation, regardless of statistical significance (Kleinbaum, 1982; Rothman & Greenland, 1998).
Results
From information provided by teachers, it resulted that the variance (R2) of impairment in preschoolers' inhibition is explained in a 78.7% by the symptoms of ADHD, ODD and CD. Lack of emotional control is explained in 53.6% by the symptoms of ODD and of ADHD-I, while the ADHD-I and the CD symptoms have no significant importance. Also, symptoms of ADHD-I explain in 82.3% impairment in the working memory of preschool children. ADHD-I, ODD, and CD symptoms proved not significant. Scale of Plan/Organize is explained in 74.7% by symptoms of ADHD-I and CD. The hyperactive type (ADHD-H) and the ODD symptoms were not significant in this case (see Table 2).
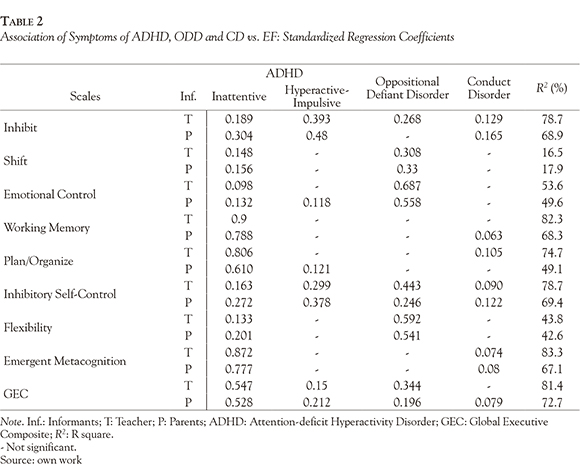
On the other hand, in the case of parents, the model explains 68.9% of inhibition. ADHD and CD symptoms are the most important in predicting inhibition, leaving aside the ODD symptoms, which have no weight within the predictive group. Emotional control is explained in 49.6% by ODD symptoms and the two types of ADHD. For its part, symptoms of CD proved not significant for emotional control. Also, the ADHD-I and the CD symptoms explained in 68.3% the working memory. In addition, symptoms of ADHD explained 49.1% of the Plan/Organize scale, while the ODD symptoms and the CD ones did not give any explanation.
Regarding the Scale of Shift, both parents and teachers reported that symptoms of ODD, in the first place, and symptoms of ADHD-I, in the second place, have greater weight to predict the scale, and explain 16.5% (according to teachers) and 17.9% (according to parents).
Finally, according to data from teachers, the combined global execution was explained 81.4% by the symptoms of the ADHD-I and those of the ODD. The ADHD-H had little weight and the CD symptoms gave no explanation. In contrast, the combined global execution reported by parents was explained 72.7% by the symptoms of ADHD, in its two types, the symptoms of ODD and the symptoms of CD.
Table 3 shows the correlations among the studied behavioural disorders, based on information from parents and teachers. It also shows the correlation among informants.
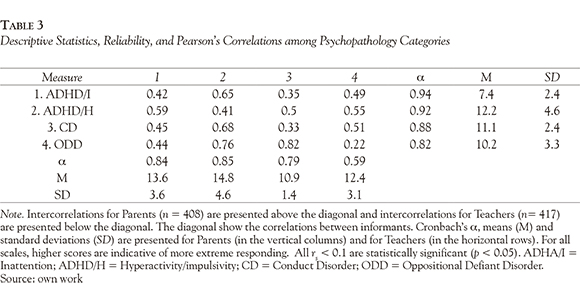
The difference between the results exposed by both informants can be explained by the relation with the child and the time spent with him. As mentioned Viñas et al. 2008, teachers compare the behaviour of the child with their peers in contexts such as the classroom and school yard; on the other hand, parents often do not concern and do not have enough time beside their children.
Discussion
This study analyses the relationship between behaviour disorders and impairments of EF, based on information provided by teachers and parents of preschool children. Thus, we agree with the literature reviewed (Brocki et al., 2010; Mullane et al., 2011) in that children with symptoms of ADHD-I have more EF impairments than other children with other symptoms. These are children who do not pay attention to events that happen around them and do not perform in an appropriate manner in their immediate context. They are unable to direct their behaviours to achieve a specific purpose. They have no initiative to plan, organize, and develop strategies to solve a problem. This information may be an additional contribution to current research on ADHD-I care about providing an appropriate term to describe the group of symptoms that represent only inattention (Carlson & Mann, 2002; Derefinko et al., 2008; Garner, Marceaux, Mrug, Patterson, & Hodgens, 2010; Harrington & Waldman, 2010). The strong association shown between ADHD and EF coincides with recent research on the subject, that define ADHD as a disorder of EF, as it is known that deficiencies in executive functioning are one of the major impairments that characterize children with ADHD and prevent them from social relations and an efficient optimal school performance (Barkley, 1998; Brown, 2006).
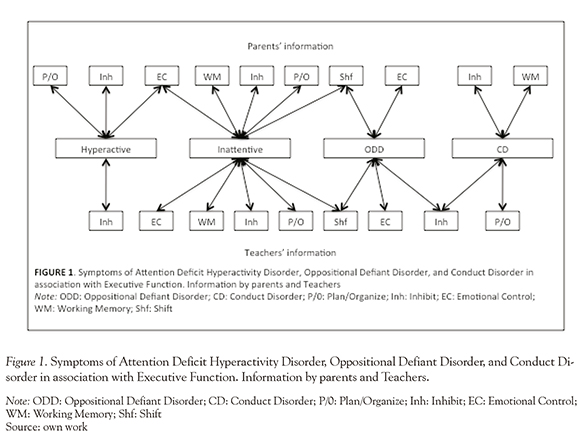
However, it can be observed a strong association between ODD and CD symptoms and deficits in EF. Figure 1 shows the different associations that exist between the disruptive behaviour disorders and the EF.
With regard to working memory, our results do not coincide entirely with the studies conducted by authors like Brocki et al. (2010) and Re et al. (2010), who claim that it is possible to note deficits in the working memory of children with disruptive behaviour disorders. We found a closer relationship between deficits in this area in children with ADHD-I symptoms and those with CD symptoms. This could be explained by considering the following example: in a classroom, both the child with symptoms of inattention, as well as the child with symptoms of CD, does not pay attention to the given instructions. This is because the child with symptoms of inattention does not give importance, perhaps does not even hear, to which has been given, therefore he does not retain in his mind the information to make it actively effective. The same applies to the child with symptoms of CD for whom it is often irrelevant what other people will propose or request.
With regard to processes such as plan/organize, according to information from parents, it was found that children with symptoms of ADHD-I or ADHD-H find it difficult to make plans of action to achieve their goals. Thus, the difficulties in planning and organizing that show children with symptoms of inattention, as well as the problems in working memory mentioned above, result in a more general deficit in the emergent metacognition. This does not happen to children with symptoms of inattention. However, it does happen to children with symptoms of CD, since this area of the second order corresponds to the ability of the child to cognitively manage tasks and use the information in working memory to guide their performance or behaviour. Thus, we agree with previous studies (Fischer et al., 2005; Wâhlstedt et al., 2008) in which it was found that children with symptoms of ADHD are affected in this area as a result of a lack of working memory skills linked to a poor ability to plan and organize activities in their daily lives. We do not agree with other studies (Raaijmakers et al., 2008; Sergeant et al., 2002; Van Goozen et al., 2004) that indicate that there was no significant deficiency of these executive activities in children with CD and ODD symptoms, unless symptoms of comorbid ADHD were found (Thorell & Wâhlstedt, 2006).
Again, from the information provided by parents and teachers, we agree with Brocki et al. (2010), Clark et al. (2002) and Sonuga-Barke et al. (2002) in that children with ADHD symptoms, in its two types, show impairments in controlling their emotions. Furthermore, we found that symptoms of inattention are also associated with problems in flexibility to switch from one activity to another when pursuing the same goal. They also have difficulty in adopting different perspectives on the same situation at different times and, finally, they have difficulty controlling their emotions. These actions lead children to persist in a wrong way to solve problems. The same applies to children with ODD symptoms, as in Sergeant et al. (2002) and Raaijmakers et al. (2008) studies. However, we do not agree with these authors in that children with CD also have problems in this process. Our results do not indicate significant executive deficits in children with symptoms of this disorder.
Lack of impulse control is one of the main features of disruptive behaviour disorders (Barkley, 1998). In this study we found that, according to teachers, children with ADHD symptoms, in its two types, with symptoms of CD and with ODD symptoms, have difficulty inhibiting their behaviour at the right time. It leads to difficulties of second order like inhibitory self-control, which is derived from the executive difficulties for impulse control and emotional control. This agrees with the literature reviewed (Fischer et al., 2005; Gambin & Swiçcicka, 2009; Qian et al., 2010; Sonuga-Barke et al., 2002; Wâhlstedt et al., 2008) in that this is one of the most affected characteristics in children with disruptive behaviour disorders, especially with ADHD. Parents gave no information about impairments in children with symptoms of ODD. Other authors such as Mahone and Hoffman (2007) in their study of preschool children with ADHD found no significant deficits in inhibitory control.
As for the global execution scale, we agree with the other mentioned researches (Fischer et al., 2005; Sergeant et al., 2002; Van Goozen et al., 2004) in that both parents and teachers say that children with disruptive behaviour disorders symptoms generally show impairments in EF, although, according to information provided by teachers, children with symptoms of CD show fewer impairments in their EF. This is explained considering that a child with symptom of CD breaks the rules by the lack of ability that has to stop or control his impulses, but is able to achieve an end, with good use of the rest of his executive processes.
Thus, we conclude that children with symptoms of ADHD, ODD, and CD have different dysfunctions in executive processes, even when there is a global impairment of EF in children with these symptoms.
The high prevalence of disruptive behaviour disorders in preschool children shows the need for clinical intervention techniques from early ages to prevent future emotional and behavioural problems (Biederman et al., 2004). As previous studies argue (Goldberg, 2002; Isquith et al., 2005; Trujillo & Pineda, 2008), children develop, during preschool level, executive processes that help them cope with their environment. These processes will reach their full maturity years later (Goswami, 2002). Assessing executive functioning in preschool can help fostering the proper development of these executive skills in children. Also important is the early detection of psychiatric symptoms, it is known that the late diagnosis can trigger greater school difficulties, social and family in the future. With this, prevention and treatment of behavioural problems from an early age are necessary to a better prognosis. Furthermore, knowing the executive deficits related to the presence of ADHD, CD or ODD symptoms will help professionals to implement programmes in preschool to develop executive skills of children with behaviour problems in a more personalized way, depending on the symptoms of the disorder they have. It will allow them to deal appropriately with context on the basis of their own characteristics.
There are many similarities between our study and others previously conducted. We agree with Espy et al. (2011) on the need for further evaluation and measurement of EF in preschoolers. They claim that the study of EF should be complemented with laboratory neurological tests to deepen the assessment of EF. Nevertheless, recently, Barkley and Fischer (2011) showed that self-reports of EF are capable of measuring deficits in daily activities and in children's functioning, so they can be used for research without using tests. To this end, the best strategy is probably to combine the use of standardised tests with laboratory tests that define what each of them measures.
A limit within this study was the lack of cases with clinically diagnosed disruptive behaviour disorders. We consider it necessary for future research to carry out longitudinal studies that assess the EF and observe both general and clinical populations. Also, consider other variables related to the development of children, as they could be parenting, attachment and socio emotional factors.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders: DSM-IV-TR (4th ed., text revision). Washington, DC: Author. [ Links ]
Anderson, P. (2002). Assessment and development ofexecutive function (ef) during childhood. Child Neuropsychology, 8(2), 71-82. http://dx.doi.org/10.1076/chin.8.2.71.8724 [ Links ]
Barkley, R. A. (1998). Attention-deficit hyperactivity disorder: A handbook fordiagnosis and treatment (2nd ed.). New York: Guilford Press. [ Links ]
Barkley, R. A. (2000). Genetics of childhood disorders: XVII. ADHD, Part 1: The executive functions and ADHD. Journal of the American Academy of Child & Adolescent Psychiatry, 39(8), 1064-1068. http://dx.doi.org/10.1097/00004583-200008000-00025 [ Links ]
Barkley, R. A., & Fischer, M. (2011). Predicting impairment in major life activities and occupational functioning in hyperactive children as adults: Self-Reported Executive Function (EF) Deficits Versus EF Tests. Developmental Neuropsychology, 36(2), 137-161. http://dx.doi.org/10.1080/87565641.2010.549877 [ Links ]
Biederman, J., Monuteaux, M. C., Doyle, A. E., Seidman, L. J., Wilens, T. E., Ferrero, F., ... Faraone, S. V. (2004). Impact of executive function deficits and attention-deficit/hyperactivity disorder (ADHD) on academic outcomes in children. Journal of Consulting and Clinical Psychology, 72(5), 757-766. http://dx.doi.org/10.1037/0022-006X.72.5.757 [ Links ]
Bonillo, A., Araujo, E., Jané-Ballabriga, M. C., Capdevila, C., & Riera, R. (2011). Brief report: Validation of Catalan version of BRIEF-P. Child Neuropsychology, 1-9. http://dx.doi.org/10.1080/09297049.2011.613808 [ Links ]
Brocki, K. C., Eninger, L., Thorell, L. B., & Bohlin, G. (2010). Interrelations between executive function and symptoms of hyperactivity/impulsivity and inattention in preschoolers: A two year longitudinal study. Journal of Abnormal Child Psychology,38(2), 163-171. http://dx.doi.org/10.1007/s10802-009-9354-9 [ Links ]
Brown, T. E. (2006). Trastorno por déficit de atención: una mente desenfocada en niños y adultos. Barcelona: Masson. [ Links ]
Carlson, C. L., & Mann, M. (2002). Sluggish cognitive tempo predicts a different pattern of impairment in the attention deficit hyperactivity disorder, predominantly inattentive type. Journal of Clinical Child and Adolescent Psychology, 31(1), 123-129. http://dx.doi.org/10.1207/153744202753441738 [ Links ]
Clark, C. A., Pritchard, V. E., & Woodward, L. J. (2010). Preschool executive functioning abilities predict early mathematics achievement. Developmental Psychology, 46(5), 1176-1191. http://dx.doi.org/doi:10.1037/a0019672 [ Links ]
Clark, C., Prior, M., & Kinsella, G. (2002). The relationship between executive function abilities, adaptive behaviour, and academic achievement in children with externalising behaviour problems. Journal of Child Psychology and Psychiatry, 43(6), 785-796. http://dx.doi.org/10.1111/1469-7610.00084 [ Links ]
Derefinko, K. J., Adams, Z. W., Milich, R., Fillmore, M. T., Lorch, E. P., & Lynam, D. R. (2008). Response style differences in the inattentive and combined subtypes of attention-deficit/hyperactivity disorder. Journal of Abnormal Child Psychology, 36(5), 745-758. http://dx.doi.org/10.1007/s10802-007-9207-3 [ Links ]
Espy, K. A., Sheffield, T. D., Wiebe, S. A., Clark, C. A. C., & Moehr, M. J. (2011). Executive control and dimensions of problem behaviors in preschool children. Journal of Child Psychology and Psychiatry, 52(1), 33-46. http://dx.doi.org/10.1111/j.1469-7610.2010.02265.x [ Links ]
Fischer, M., Barkley, R. A., Smallish, L., & Fletcher, K. (2005). Executive functioning in hyperactive children as young adults: Attention, inhibition, response Perseveration, and the impact of comorbidity. Developmental Neuropsychology, 27(1), 107-133. http://dx.doi.org/10.1207/s15326942dn2701_5 [ Links ]
Gambin, M., & Swiçcicka, M. (2009). Relation between response inhibition and symptoms of inattention and hyperactivity-impulsivity in children. British Journal of Clinical Psychology, 48(4), 425-430. http://dx.doi.org/10.1348/014466509X449765 [ Links ]
Garner, A. A., Marceaux, J. C., Mrug, S., Patterson, C., & Hodgens, B. (2010). Dimensions and correlates of attention deficit/hyperactivity disorder and sluggish cognitive tempo. Journal of Abnormal Child Psychology, 38(8), 1097-1107.http://dx.doi.org/10.1007/s10802-010-9436-8 [ Links ]
Gioia, G., Espy, K., & Isquith, P. K. (2003). BRIEF-P: Behavior Rating Inventory of Executive Function-Preschool Version: Professional Manual. Lutz, FL: Psychological Assessment Resources. [ Links ]
Goldberg, E. (2002). El cerebro ejecutivo: lóbulos frontales y mente civilizada. Barcelona: Crítica. [ Links ]
Goswami, U. (2002). Blackwell handbook of childhood cognitive development. Malden, MA: Blackwell Publishers. [ Links ]
Harrington, K. M., & Waldman, I. D. (2010). Evaluating the utility of sluggish cognitive tempo in discriminating among DSM-IV ADHD subtypes. Journal of Abnormal Child Psychology, 38(2), 173-184. http://dx.doi.org/10.1007/s10802-009-9355-8 [ Links ]
Isquith, P. K., Crawford, J. S., Espy, K. A., & Gioia, G. A. (2005). Assessment of executive function in preschool-aged children. Mental Retardation and Developmental Disabilities Research Reviews, 11(3), 209-215. http://dx.doi.org/10.1002/mrdd.20075 [ Links ]
Kleinbaum, D. G. (1982). Epidemiologic research: Principles and quantitative methods. New York: John Wiley & Sons. [ Links ]
Mahone, E. M., & Hoffman, J. (2007). Behavior ratings of executive function among preschoolers with ADHD - PB - Psychology Press. The Clinical Neuropsychologist, 21(4), 569-586. http://dx.doi.org/10.1080/13854040600762724 [ Links ]
Mattison, R. E., & Mayes, S. D. (2012). Relationships between learning disability, executive function, and psychopathology in children with ADHD. Journal of Attention Disorders, 16(2), 138-146. http://dx.doi.org/10.1177/1087054710380188 [ Links ]
Mullane, J. C., Corkum, P. V., Klein, R. M., McLaughlin, E. N., & Lawrence, M. A. (2011). Alerting, orienting, and executive attention in children with ADHD. Journal of Attention Disorders, 15(4), 310-320. http://dx.doi.org/10.1177/1087054710366384 [ Links ]
Qian, Y., Shuai, L., Cao, Q., Chan, R. C. K., & Wang, Y. (2010). Do executive function deficits differentiate between children with Attention Deficit Hyperactivity Disorder (ADHD) and ADHD - comorbid with Oppositional Defiant Disorder? A cross-cultural study using performance-based tests and the Behavior Rating Inventory of Executive Function. The Clinical Neuropsychologist, 24(5), 793-810. http://dx.doi.org/10.1080/13854041003749342 [ Links ]
Raaijmakers, M. A. J., Smidts, D. P., Sergeant, J. A., Maassen, G. H., Posthumus, J. A., Engeland, H., & Matthys, W. (2008). Executive functions in preschool children with aggressive behavior: Impairments in inhibitory control. Journal of Abnormal Child Psychology, 36(7), 1097-1107. http://dx.doi.org/10.1007/s10802-008-9235-7 [ Links ]
Re, A., De Franchis, V., & Cornoldi, C. (2010). Working memory control deficit in kindergarten ADHD children. Child Neuropsychology, 16(2), 134-144. http://dx.doi.org/10.1080/09297040903373404
Rothman, K. J., & Greenland, S. (1998). Modern epidemiology (2nd ed.). Lippincott Williams & Wilkins. [ Links ]
Schoemaker, K., Bunte, T., Wiebe, S. A., Espy, K. A., Dekovic, M., & Matthys, W. (2012). Executive function deficits in preschool children with ADHD and DBD. Journal of Child Psychology and Psychiatry, 53(2), 111-119. http://dx.doi.org/10.1111/j.1469-7610.2011.02468.x [ Links ]
Senn, T. E., Espy, K. A., & Kaufmann, P. M. (2004). Using path analysis to understand executive function organization in preschool children. Developmental Neuropsychology, 26(1), 445-464. http://dx.doi.org/10.1207/s15326942dn2601_5 [ Links ]
Sergeant, J. A., Geurts, H., & Oosterlaan, J. (2002). How specific is a deficit of executive functioning for attention-deficit/hyperactivity disorder? Behavioural Brain Research, 130(1-2), 3-28. doi:10.1016/S0166-4328(01)00430-2 [ Links ]
Sonuga-Barke, E. J. S., Dalen, L., Daley, D., & Remington, B. (2002). Are planning, working memory, and inhibition associated with individual differences in preschool ADHD - symptoms? Developmental Neuropsychology, 21(3), 255-272. http://dx.doi.org/10.1207/S15326942DN2103_3 [ Links ]
Sprafkin, J., & Gadow, K. D. (1996). Early childhood symptom inventories manual. Stony Brook, NY: Checkmate Plus. [ Links ]
Thorell, L. B., & Wâhlstedt, C. (2006). Executive functioning deficits in relation to symptoms of ADHD and/or ODD in preschool children. Infant and Child Development, 15(5), 503-518. http://dx.doi.org/10.1002/icd.475 [ Links ]
Trujillo, N., & Pineda, D. (2008). Función ejecutiva en la investigación de los trastornos del comportamiento del niño y del adolescente. Revista Neuropsicología, Neuropsiquiatria y Neurociencias, 8(1), 77-94. [ Links ]
Van Goozen, S. H. M., Cohen-Kettenis, P. T., Snoek, H., Matthys, W., Swaab-Barneveld, H., & van Engeland, H. (2004). Executive functioning in children: A comparison of hospitalised ODD and ODD/ ADHD children and normal controls. Journal of Child Psychology and Psychiatry, 45(2), 284-292. http://dx.doi.org/10.1111/j.1469-7610.2004.00220.x [ Links ]
Viñas, F., Jané, M. C., Canals, J., Esparó, G., Ballespí, S., & Domènech-Llaberia, E. (2008). Evaluación de la psicopatología del preescolar mediante el Early Childhood Invetory-4 (ECI-4): concordancia entre padres y maestros. Psicothema, 20(3), 481-486. [ Links ]
Wâhlstedt, C., Thorell, L. B., & Bohlin, G. (2008). ADHD - symptoms and executive function impairment: Early predictors of later behavioral problems. Developmental Neuropsychology, 33(2), 160. http://dx.doi.org/10.1080/87565640701884253 [ Links ]
Welsh, M. C., Pennington, B. F., & Groisser, D. B. (1991). A normative-developmental study of executive function: A window on prefrontal function in children. Developmental Neuropsychology, 7(2), 131-149. [ Links ]
