











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Sinus histiocytosis with massive lymphadenopa-thy, also known as Rosai-Dorfman disease, was first described by Rosai and Dorfman in 1969. It is a rare histiocytic proliferative disorder of unknown etiology 1, and different cell populations and cytokines are involved in its pathogenesis. The participation of inflammatory cytokines such as macrophage colony stimulating factor, IL-1 ß, IL-6, and TNF-α is common 2.
This disease predominantly affects children and young adults in the first 2 decades of life, particularly males. Patients who present with extranodal disease may require systemic therapy, for which there is currently no standardized regimen to date. Systemic therapies include corticosteroids, mTOR inhibitors, radiation therapy, chemotherapy, and immunomodulatory therapy.
CASE DESCRIPTION
A 33-year-old mestizo man from Cartagena -Colombia, who works as a street vendor, of low economic status, without a relevant medical history, consulted due to the presence of a progressive deformity in the right frontal side of the face and pain of 6 months of evolution with slow progression and no other associated symptoms.
On physical examination, he presented with growth of the right frontal region, without the presence of dermatological lesions, lymph-adenopathy or visceromegaly. Complementary laboratory tests (complete blood count, blood chemistry, sedimentation rate, C-reactive protein, proteinogram, immunoglobulins, complement, ANA, VDRL, hepatitis and HIV, beta-2-microglobulin and chest radiography) were performed, which were normal or negative. Initial imaging studies showed extensive inflammatory/infectious bone involvement, which led to suspect osteomyelitis as the first diagnostic possibility (Figure 1).
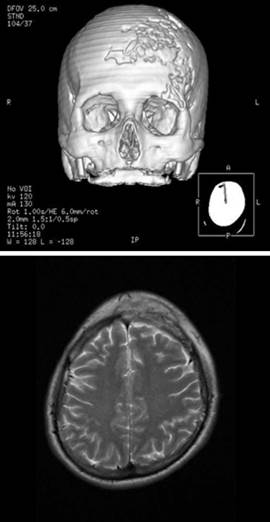
Source: Document obtained during the study.
Figure 1 Initial imaging studies of the lesion showing extensive inflammatory bone involvement, with osteomyelitis as the first diagnostic possibility.
The histopathological study revealed histiocyte sheets at the frontal bone level with clear cytoplasm and rounded nuclei, without significant atypia, lymphocyte and neutrophil emperipolesis, positivity for CD68 and S100, and negativity for CD1a in immunohistochemistry (Figure 2). The microbiological study was negative for fungi, M. tuberculosis, atypical mycobacteria and Leishmania sp. These findings led to the diagnosis of extranodal Rosai-Dorfman disease with isolated bone involvement; an extension study was carried out, but no systemic affectation was detected.
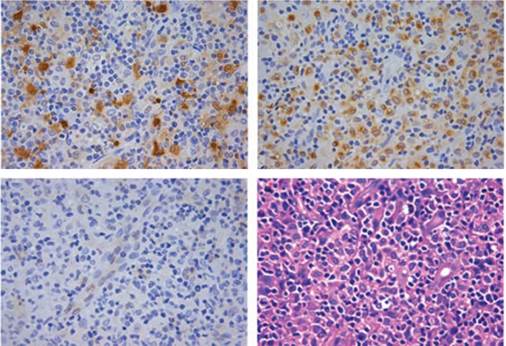
Source: Document obtained during the study.
Figure 2 The histopathological study showed histiocyte sheets with clear cytoplasm and rounded nuclei, without significant atypia and lymphocyte and neutrophil emperipolesis. Positivity for CD68 and S100 and negativity for CD1a were found in immunohistochemistry stains.
Given the possibility of having a self-limited course (50% of cases), medical follow-up was provided for a period of 2 months without achieving improvement. As a consequence, treatment with prednisolone at 1 mg/kg/day was started for 2 months, without obtaining a positive response, so methotrexate 15 mg/week was initiated with evident improvement, from a clinical perspective, after 2 months due to the improvement of the deformity in the face and imaging scans showing partial resolution of the initial tomographic findings. Throughout the clinical follow-up, no adverse reactions to the use of steroids in conjunction with methotrexate were observed.
DISCUSSION
Rosai-Dorfman disease may occur in any age group; however, its occurrence predominates in children and young adults, particularly males. Its classic clinical presentation is characterized by the appearance of massive and indolent cervical lymphadenopathy with fever, hypergammaglobulinemia and increased erythrocyte sedimentation rate 3. The reported patient did not have these characteristics since local bone involvement predominated at the level of the cranial vault, being initially managed as an infectious process.
RDD is a benign histiocytic proliferative disorder, with a prevalence of 1:200 000 and an estimated 100 new cases per year in the United States. Its form may be nodal or extranodal. In cases of nodal disease, cervical lymphadenopathy is the most frequent, followed by axillary, inguinal and mediastinal location. On the other hand, extranodal forms usually affect the central nervous system, skin, soft tissues, bone, oral cavity, and salivary glands 2. Extranodal involvement is frequent and occurs in 43% of patients, mainly in the head and neck. Isolated extranodal presentation may also occur, as in the case of our patient 1.
Isolated bone involvement is a rare manifestation of the disease, occurring in less than 10% of the cases 4. The most common symptoms in this scenario are pain and swelling. Data available in the reviewed literature states that the skull, face and long bones are the most affected areas, with lytic lesions predominantly 4. In contrast to the benign course of nodal manifestations, Rosai-Dorfman disease in the bones has a poorer prognostic factor, as it tends to have a chronic course with frequent relapses.
Imaging scans are useful for the identification, staging and monitoring of the clinical course of the disease with bone involvement. However, this disease may simulate other conditions, including neoplasms (lymphoma, Kaposi's sarcoma, metastasis and malignant histiocytosis) and inflammatory conditions (infections: tuberculosis and histiocytosis; non-infectious granulomatous conditions: Castleman disease, granulomatosis and sarcoidosis) 1. In the present case, scans were interpreted as initially associated with a local infectious process, for which the patient received a course of antibiotics that was suspended based on histological findings.
The course of this disease is usually benign, with frequent cases of spontaneous regression; less than 10% of patients suffer progressive disease associated with adverse outcomes, including death. In most cases documented in the literature, patients usually receive surgical or glucocorticoid-based management. Several treatments, such as systemic corticosteroids, surgery, chemotherapy and radiotherapy, or a combination of these, have been reported, all with variable efficacy 5. Vincristine and imatinib 6 have demonstrated it to be effective in refractory patients. There have also been reports of patients who responded well to low dosages of methotrexate 7.
Timely diagnosis and treatment based on the descriptions found in the literature allowed for the improvement of the patient's condition, who was previously isolated from his family and social group due to the lack of knowledge on his disease.
CONCLUSION
Extranodal Rosai-Dorfman disease is common; however, isolated bone involvement is rare, accounting for less than 10% of cases. This is an extremely rare disease that poses a diagnostic challenge considering that its clinical suspicion is based on its traditional form of presentation, which was not observed in our patient. In this case, histology and immunohistochemical studies were essential to reach the diagnosis.

